





Abstract
Epithelioid angiosarcoma is a rare, highly malignant tumour with a poor prognosis. We present the case of a 75 year old man who underwent an incision biopsy to diagnose the soft tissue tumour and suffered from surgically uncontrollable haemorrhage. The case report demonstrates the value of interventional radiology for acute bleeding and radiotherapy for more chronic tumour bleeding.
INTRODUCTION
Epithelioid angiosarcoma is a rare, highly malignant tumour with a poor prognosis. The following case report highlights a potentially life threatening complication of undertaking an incision biopsy on a soft tissue tumour, namely surgically uncontrollable haemorrhage from an unsuspected vascular lake. The case report demonstrates the value of interventional radiology for acute bleeding and radiotherapy for more chronic tumour bleeding.
CASE REPORT
A 75 year old male presented with a 3 month history of painful progressive left buttock swelling and non-productive cough. Past medical history included carcinoma of the prostate 5 years previously, which had been treated with surgery and radiotherapy. Examination revealed a fixed 10 by 10 cm mass in the left buttock extending over the sacro-iliac joint. Examination of the chest revealed a large, right-sided pleural effusion. Investigations included a chest CT which confirmed the pleural effusion and some pleural plaques. A pleural aspiration cytology confirmed a malignant effusion, although did not differentiate the cell type.
The pelvic MRI scan demonstrated a large 10 x 10 x 5cm heterogeneous lesion in the left buttock, occupying much of the posterior portion of the gluteus maximus and invading the iliac bone and sacrum. Appearances were highly suggestive of a soft tissue sarcoma. This was also evident on a staging CT of the abdomen. The primary lesion was not operable and the presence of the malignant effusion denoted stage 4 disease, (T2, N0, M1).
Percutaneous needle core biopsy of the lesion was inconclusive and incision biopsy was requested after drainage and talc pleurodesis of the pleural effusion.
At the time of incision biopsy the capsule of the lesion was incised over a small area. This resulted in profuse bleeding from a deep, fresh blood filled, cavity within the cystic tumour. A large vascular lake in the centre of the tumour was evident with a significant vascular flow rate. The cavity was therefore tightly packed with haemostatic material and firm pressure applied to the wound, causing partial cessation of the haemorrhage. Full surgical control of the bleeding was not possible due to the fact that the tumour was in-operable and the feeding vessels originated from the internal iliac vessels running through the invaded bone of the ileum. Urgent angiography and embolisation was therefore performed.
Angiography revealed a tumour blush in the gluteal region supplied by the median sacral artery and the posterior division of the internal iliac artery (IIA). The IIA was catheterised revealing multiple feeding branches with extravasation from one (Figure 1).
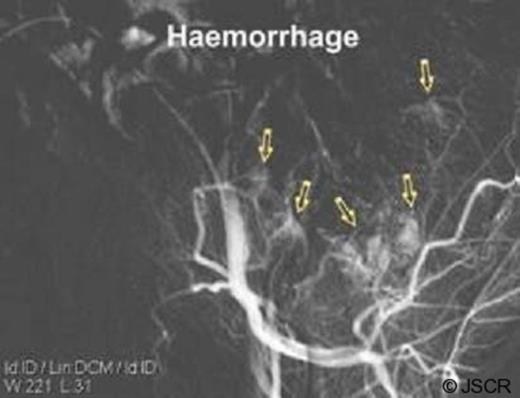
Angiograms pre-embolisation with Histo-acryl

Angiograms post-embolisation with Histo-acryl
Over the ensuing 3 weeks, despite the initial successful embolisation the patient haemorrhaged on a further 2 occasions despite pressure dressings to the wound area. On both of these occasions further embolisation was undertaken with initial successful outcome. On each occasion, a different set of feeding vessels was noted to be bleeding and was embolised.
Histology from the incision biopsy revealed a diagnosis of epithelioid angiosarcoma (Figure 2) which is known to be associated with the development of vascular lakes.
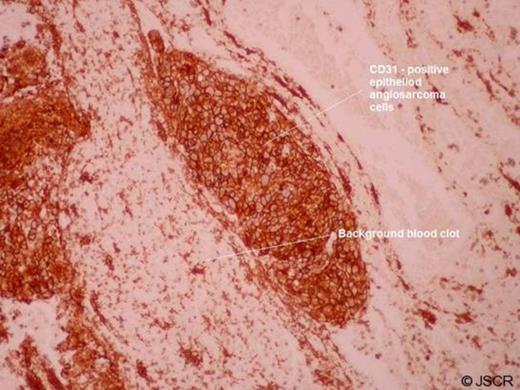
(CD31 immunohistochemistry: Immunoperoxidase, original magnification x100)
To prevent the occurrence of further haemorrhage, the patient was given a course of radiotherapy (30Gy in 10 treatments over 14 days).
No further haemorrhage occurred and the patient was discharged for rehabilitation. Palliative chemotherapy to control respiratory symptoms from the pleural effusion was declined and the patient died 6 months after initial presentation.
DISCUSSION
The epithelioid phenotype of angiosarcoma was first described in 1976 by Rosai and colleagues who documented cases of cutaneous angiosarcomas. It was later documented by Fletcher and colleagues in 1991 who described deeper lesions found in the soft tissues where they are now most commonly found. (1)
Epithelioid angiosarcomas are rare, high-grade, malignant, vascular tumours, which have an aggressive course and tend to recur locally, spread widely, and have a high rate of lymph node and systemic metastases.(2) It often presents in middle-aged and elderly males with a peak incidence in the seventh decade of life. Prognosis for these types of tumours is very poor with death usually occurring from 6 months to 2 years after presentation.
Epithelioid angiosarcomas have been described arising in various soft tissues around the body and are most often metastatic in origin. Such areas include lungs, thyroid, limb girdle and retroperitoneum. Metastatic lesions have even been found in the oral cavity.
Histologically these tumours consist of solid and infiltrative sheets of epithelioid cells characterised by large, oval to round cells with abundant eosinophilic cytoplasm, vesicular nucleus and eosinophilic nucleolus.(3)
In most cases there are vascular channels or cystically dilated spaces. Vascular lakes are therefore a common finding associated with these types of sarcoma. A distinctive “starry-sky” histological pattern has also been reported in epithelioid angiosarcomas. Immunohistochemically the neoplastic cells show positivity for endothelial cell markers such as CD31, CD34, factor VIII-related antigen, and vimentin.(4-5)
Due to cytokeratin expression and epithelioid growth pattern these tumours can occasionally be misdiagnosed as carcinomas. Endothelial differentiation can be confirmed ultrastructually by the presence of Weibel-Palade bodies, intermediate filaments and basal lamina. Intracytoplasmic vacuoles containing red blood cells are often present in some cells.(4)
Irradiation of soft tissues for the treatment of various primary cancers is well documented as a cause for several types of sarcoma. As in this case, the patient had undergone a course of radiotherapy for prostate cancer several years prior to presenting with the pelvic sarcoma and this therefore may have been the causative factor. Other risk factors for the development of angiosarcomas include carcinogens, chronic lymphoedema and hormonal status. There are very few cases in the literature of pelvic epithelioid angiosarcoma. However one such case documented a lesion of the mons pubis 4 years following radiotherapy for vulval carcinoma.(5)
Angiography and tumour embolisation is a well established treatment of tumours both pre- and post-operativley. Tumour embolisation may be carried out for acute bleeding from tumour vessels, and to reduce the blood supply to tumours prior to surgery. Palliative radiotherapy can be used effectively in the treatment of bleeding from advanced tumours. The most common tumours, where bleeding occurs, are pelvic and lung malignancies. Treatment usually consists of delivering one or two fractions of 5-8 Gy each on successive days. The patient may require blood transfusions during treatment.

{kind=link}
{kind=link}
{kind=link}