





Abstract
Giant ureteric calculi are extremely rare in children. We present a case of a child who was originally admitted for observation following non-accidental injury and had an episode of painless haematuria as an inpatient. Ultrasonography demonstrated left hydronephrosis and a 2cm echogenic area in the proximal ureter. A plain abdominal radiograph surprisingly revealed two left ureteric calculi, one 7cm and the other 4cm in length. Stone extraction was achieved using an open left ureterolithotomy and pyelolithotomy.
INTRODUCTION
Renal tract calculi in children are an uncommon occurrence. Giant ureteric calculi are even more rare and can present in different ways. Ultrasonography is currently used as the initial investigation for suspected renal tract calculi. The authors present a case of giant ureteric calculus highlighting the importance of plain film radiograph in the assessment of children with suspected renal tract calculi.
CASE PRESENTATION
A 7-year-old boy was admitted for observation following non-accidental injury. He had an episode of painless haematuria as an inpatient. There was no history of urinary tract infections or renal colic. Clinical examination was unremarkable. Urine culture showed no growth and blood investigations were normal. Ultrasonography demonstrated left hydronephrosis and a 2cm echogenic area with acoustic shadow in the proximal ureter, consistent with a ureteric calculus. Plain radiography astonishingly revealed a large 7cm radio-opaque shadow in the line of the left ureter extending from the left pelvi-ureteric junction to the mid-ureter, and a second 4cm opacity in the left distal ureter (Fig 1).

Plain abdominal radiograph demonstrating large opacity extending from the left pelvi-ureteric junction to the mid ureter, and a smaller opacity in the distal ureter.
A DMSA scan showed split renal function of 30% on the left side and 70% on the right. Underlying metabolic abnormalities associated with stone formation were excluded. A dilated left ureteric orifice was seen on cystoscopy. The left distal ureter was identified using an extraperitoneal approach through a left iliac fossa incision. The distal calculus was extracted through a longitudinal ureteric incision. As it was not possible to retrieve the proximal stone through this incision, a pyelolithotomy was performed using a further left flank incision. The proximal ureteric calculus measured 6.5 x 1.8 cm and weighed 7991 milligrams (Fig 2).
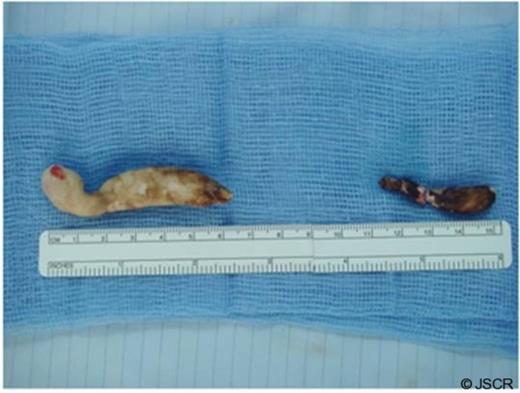
Ureteric calculi removed from the proximal (left ) and distal (right) ureter.
It was composed of 85% magnesium ammonium phosphate (struvite) and 15% carbonate apatite. The distal calculus measured 3cm in length. The patient made an uneventful recovery and is under regular follow up.
DISCUSSION
The UK incidence of urolithiasis in children has been estimated to be two per million per annum (1). Ureteric stones greater than 5 cm in length are termed ‘giant’. Renal tract calculi commonly present with renal colic, haematuria, urinary tract infections or lower urinary tract symptoms. Giant ureteric calculi have been reported to present with urinary tract infection and retention of urine (2,3). They can however be asymptomatic and progress silently, as was characterised by our case, where the giant calculus was discovered incidentally.
Current practice reflects evidence that ultrasonography is more sensitive than plain radiography in detecting renal tract calculi in children (4,5). Ultrasonography is used as an initial investigation for suspected renal tract calculi. However, ultrasonography is less sensitive in detecting and characterising ureteric stones than plain radiography. A combination of ultrasonography and plain radiography has therefore been recommended as the standard assessment. The present case highlights the importance of performing a plain radiograph. Ultrasonography does not always accurately characterise ureteric calculi and if a plain radiograph had not been performed, the extent of the calculus would not have been appreciated and a different course of management may have been undertaken.
The management of giant ureteric calculi entails removal of the calculus or nephroureterectomy depending on kidney function. Endourological procedures for giant ureteric calculi would prove difficult.
The authors wish to emphasise the importance of including a plain abdominal radiography in the pre-operative assessment of ureteric calculus in children.

{kind=link}
{kind=link}