





Abstract
Congenital hand and forearm anomalies pose a unique challenge in plastic and pediatric surgery. We present a case report of an 8-months-old girl with a congenital left sided hand and forearm anomaly, provisionally diagnosed as atypical left mirror hand anomaly. Classically there is absence of radius and duplication of ulna; however, our case had normal radius and ulna and a hand with seven digits arranged in two groups. We did a surgery which involved a ray amputation of the finger ulnar to the most radial digit, aiming to preserve an adequate first web space to reconstruct the thumb. The result of the surgical treatment in both functional and cosmetic aspects was, in authors’ opinion, good.
Introduction
Mirror hand deformity is a rare congenital deformity in which there is an absent thumb as well as mirror image duplication of the fingers; there is usually a deep cleft separating the ulnar fingers from the radial ones.
Mirror hand deformity is classified into two main types according to the bones of the forearm: The classic type (also known as ulnar dimelia) in which the forearm contains two ulnae and the non-classic type in which the forearm contains a radius and one or two ulnae [1].
Pathogenesis of ulnar dimelia is related to the upper limb embryology. The development of the radio-ulnar plane of the limb is controlled by a group of mesenchymal cells called the zone of polarizing activity [2].
The primary event results in failure of the radial ray to develop. The ulnar area will then induce the differentiation of two groups of ulnar rays [3].
The presence of two ulnae means that there can be no radio-ulnar joints, which means the rotation of the forearm is very limited; movements of the wrist and elbow are also restricted in many cases, however. The non-classical type may present with normal movement of the elbow, wrist and forearm as it contains normal radius [4].
The main functional problems that need to be resolved are the stiff elbow and the polydactylous hand which often requires surgery [5].
This case is reported because of the extreme rarity of the condition.
Case report
We are reporting a case of ulnar dimelia in an 8-months-old girl and the subsequent successful surgery of this deformity.
An 8-months-old girl: full-term, normal vaginal delivery, with normal perinatal medical history and no family history of congenital musculoskeletal anomalies presented with this congenital hand deformity since birth (Fig. 1).
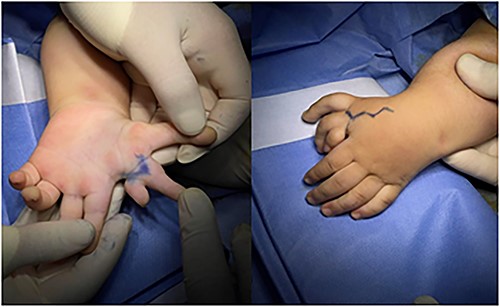
Photographs preoperatively, showing the asymmetrical mirror hand with seven digits arranged in two groups.
We find that our case was a non-classical ulnar dimelia as the patient has one radius and one ulna. The hand bears six triphalangeal digits with six corresponding metacarpals; there is also rudimentary finger that contains two bones only, which was the third finger. The wrist has two ossification centers correspondent to two capitates (Fig. 2).

Anteroposterior radiograph of the left wrist, showing one radius and one ulna, the wrist has two ossification centers, the hand bears six triphalangeal digits with six corresponding metacarpals arranged in two groups; there is also rudimentary finger that contains only two bones.
On examination all the fingers had both normal flexion and extension, supple joints with radial deviation of the wrist.
The child was prepared for surgery under general anesthesia.
We used the principles of pollicisation to reconstruct the thumb by maintaining the largest and most functional of the accessed fingers and do intrinsic muscle transfers.
We did ray amputation to finger ulnar to the most radial digit in addition to excision of the rudimentary digit to preserve adequate first web space, in addition to repair of interosseous muscles with augmentation of the interosseous power as thumb abductor by suturing of flexor tendon of the amputated digit to them, skin closure was done with vicryl suture (Fig. 3).
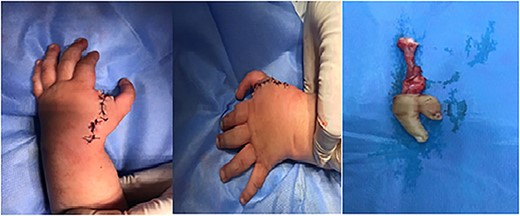
Photographs of the hand after surgery immediately.
Follow-up after 5 months reveals normal function hand (Fig. 4).

Photographs of the hand 5 months after pollicisation showing normal functiong hand.
Discussion
Duplication of the ulna is an extremely rare anomaly. The radial sided ulna is almost always hypoplastic and short and the hand is deviated to the radial side and the limb is also shorter than the contralateral side [6].
Skeletal malformation may be followed by arterial and nervous anomalies such as an absence of the radial artery, duplication of the ulnar artery, shortening of radial nerve and duplication of ulnar nerve (sometimes with collaterals to median nerve) [7], however, we didn’t find any associated anomaly.
We found the excess radial fingers are joined in a partial Syndactyl, the palm is flat without any thenar or hypothenar muscles. Just like this case report [8].
Polydactyly of ulnar dimelia differs from the ordinary supernumerary digits in several respects. The thumb is absent in ulnar dimelia replaced by two or more phalangeal digits that collectively conduct the function of opposition [9].
In our case we found that it is very important to carefully choose the best finger for pollicization. That is supported by another literature [5].
Because of the dynamic character of deformities like the mirror hand, recurrences or the appearance of associated functional and structural abnormalities may develop even after successful initial reconstruction. Therefore, it is recommended to do a long term follow-up because surgical corrections are efficient at any age though the primary operation has to be done as early as possible [8].
According to the referenced literature, the best age for the reconstruction of hand is before the second year [6].
In surgical approach to the mirror hand it is recommended to do graded surgery and to keep the limb in a long arm splint with the elbow flexed, wrist extended and thumb abducted for 4–6 weeks [10].
Conflict of interest statement
None declared.
Funding
None declared.
Data availability
The author confirms that all data generated during this study are included in this article and are available for open access.

{kind=link}
{kind=link}
{kind=link}
{kind=link}