





Abstract
Sacral neuromodulation is a minimally invasive option to manage voiding dysfunction that is refractory to conservative measures and oral pharmacotherapy. The technique involves implantation of a sacral tined lead that is connected to a pulse generator to modulate the pelvic area. The procedure is carried out over two stages. Surgical explantation of the entire device with debridement of the infected tissue is recommended in instances of infection. Nevertheless, solid reports about management of device infections or skin erosions are lacking. Thus, I present a case of a tined lead wire skin exposure in a perfectly functioning device that was salvaged with surgical reposition without complications.
INTRODUCTION
Sacral neuromodulation (SNM) with InterStim (Medtronic, Minneapolis, MN) is a minimally invasive procedure to treat refractory lower urinary tract symptoms (LUTS). The technique involves an implantable device. Device related complications are generally low. It has been suggested that explantation of the entire device with tissue debridement is recommended in instances of infection. Solid reports about management of SNM device infections or skin erosions are lacking. Herewith, I present a case of a lead wire skin exposure in a perfectly functioning SNM device that was salvaged with surgical reposition without complications.
CASE REPORT
A 23-year-old lady presented in May 2013 with non-febrile recurrent urinary tract infections (UTIs) and LUTS mainly failure to empty in nature. She used to empty with straining. She was otherwise healthy apart from obesity. Urodynamics confirmed poor detrusor contractility and high post voiding residual in which straining was not adequate to empty properly. She was started on self-clean intermittent catheterization (CIC). On follow up, she was happy and content. The recurrent UTIs subsided. In November 2016, she presented for stating that performing CIC was not convenient since she has started college and wanted to seek an alternative treatment modality, so we agreed to proceed with SNM. In April 2017, she underwent stage I SNM with InterStim device. There was >90% improvement and thus stage II was carried out. In February 2020, she presented having noticed a piece of the hardware wire eroding through the skin with minimal discomfort. Nevertheless, the device was functioning well with spontaneous voiding. The patient noted that she underwent sleeve gastrectomy in 2018 and lost ~70 kg. Examination revealed that part of the wire had eroded through the skin with clear exist and entry points, but no signs of induration or infection noted (Fig. 1). She was told this necessitates full explantation and an implementation of a new device. Patient was reluctant to proceed as the system was otherwise functioning perfect and was wondering if a less invasive measure can be undertaken. Since there were no signs of infection locally or systematically and after obtaining an informed consent discussing risks and benefits, we made a decision to proceed with a salvage procedure in 9 September 2020. The patient received 2 g of ceftriaxone prophylactically. Prior to incision, the operative field and wire were cleansed thoroughly with chlorhexidine and alcohol solution for 10 min. A small incision was made underneath the exposed wire revealing a clean healthy tissue (Fig. 2). Swap was sent for culture. The wire was buried back, and wound closed in two layers (Fig. 3). The wound was irrigated well with clindamycin wash throughout the procedure. She had uneventful recovery and discharged after 24 h with oral amoxicillin/clavulanic for 10 days. The swap culture showed few epithelial cells but did not grow any organism. Subsequent periodic follow ups showed a healthy wound that has healed well without any signs of infection 6 months post-surgery. Patient was happy with the outcome and her device continued to function well.

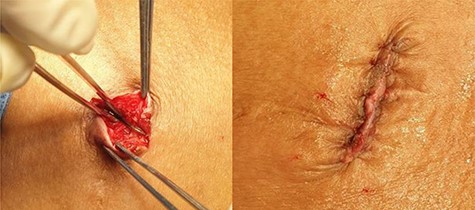
Wire eroding through the skin.

A small incision underneath the exposed wire revealing a clean healthy tissue.
The wire buried and wound closed in two layers.
DISCUSSION
This report highlights a situation that could be encountered by SNM implanters, namely a perfectly functioning device despite a skin exposure or erosion of the lead wire in the absence of frank signs of local or systemic infection. It seems to be a fair argument for attempting to salvage the device in this situation since patients may not obtain as good response should they are explanted in full and then implanted again which can be coupled by the patients’ wishes to do the minimum required if possible. With the increased number of patients implanted worldwide, it is not uncommon to encounter such situations. I have anecdotally noticed many patients having their device getting too close to skin after long time has elapsed post implantation due to extensive weight loss which could leave them with a lack of the subcutaneous tissue coverage of the device.
Tam et al. described a case of pain at the lead site secondary to wire protrusion in a patient with a slim body habitus [1]. The patient had a left-sided implant which was removed secondary to persistent pain and replaced on the contralateral side. During removal, it was noted that the most proximal tine was protruding from the skin. In a study by Hijaz et al., post-implantation challenges were examined in a series of 214 patients [2]. They observed four cases of a draining sinus from the IPG site in the absence of clear evidence of infection or positive bacterial culture. The cases were managed initially by antibiotics and relocation of the IPG into a deeper or another pocket on the contralateral side. However, they had recurrent drainage or frank infection that necessitated entire system explantation. Force et al. indicated that superficial wound dehiscence without dislodgment or exposure of the device is a complication that can usually be managed conservatively, however erosion of the stimulator through the skin is more serious and ultimately leads to device removal [3].
In my case, the absent of infection, the presence of an otherwise good functioning device and patient’ desire were the driving force to undertake such an approach. Nevertheless, such a case should not be done in all similar encounters and must be decided on a case-by-case basis. The patients must be fully informed and consented about the risks and benefits to carry out this kind of revision. They should be well informed about what is the standard of care based on common general surgical principle, guidelines, and expert opinion and what is done as an exception under specific circumstances as there are no specific published reports regarding treatment of SNM device infections [4]. In particular, the risk of subsequent infection and possible eventual explantation must be put forward and strict infection control measures must be entertained. Fortunately, my patient had uneventful recovery and follow up. The device was salvaged, skin exposure resolved completely and no complications occurred, specifically no acute or late infective shortcomings were observed over a follow up extending > 6 months.
CONFLICT OF INTEREST STATEMENT
Tariq F. Al-Shaiji has received honorarium for Medtronic sponsored lectures.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}