





Abstract
Gastric rupture due to blunt trauma is rare, occurring in only 0.07–1.2% of all abdominal blunt traumas. We reported a case with a 10-cm-long hole and review 25 cases in Japan. A 22-year-old man was involved in a traffic accident, 2 h after eating a lot of food. He had suffered muscular defense in the abdomen. An abdominal computed tomography (CT) scan revealed free air, disruption of the gastric wall and a lot of food residue. The laparotomy showed a burst of 10 cm that ran parallel to the long axis from the cardia to the body. A simple closure was primarily performed and drains were placed in the abdominal cavity. The patient was discharged on the 32nd day. Most cases of gastric rupture are diagnosed intraoperatively, but careful evaluation of CT scans and patient interviews are needed to make an accurate preoperative diagnosis.
BACKGROUND
A gastric rupture due to a blunt abdominal trauma is a rare [1–4], clinical emergency handled by physicians who are engaged in trauma patient care. Here, we present a case of traumatic gastric rupture resulting in a large rupture hole of 10 cm. We outline the steps taken to ensure a proper preoperative diagnosis and then provide a review of the Japanese literature to date.
CASE REPORT
Our case was a 22-year-old man measuring 180 cm in height and weighing 86 kg. Two hours after eating a large amount of food, he was involved in a collision between his motorcycle and a motor vehicle. At the examination, he was alert and his vital signs were stable. The patient presented with an open skull fracture on the left forehead and described muscular defense throughout the abdomen. A whole-body computed tomography (CT) scan showed an open skull fracture reaching the left skull base (Fig. 1), and free air, ascites fluid, disruption of the gastric wall and a large amount of food residue behind the spleen (Fig. 2 and b). The head wound was first treated, and then, a laparotomy was performed on suspicion of a traumatic gastric rupture.
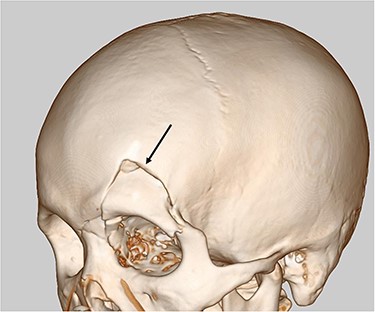
Head CT scan revealed open skull fracture reaching the left skull base (arrow) and mild brain contusion.
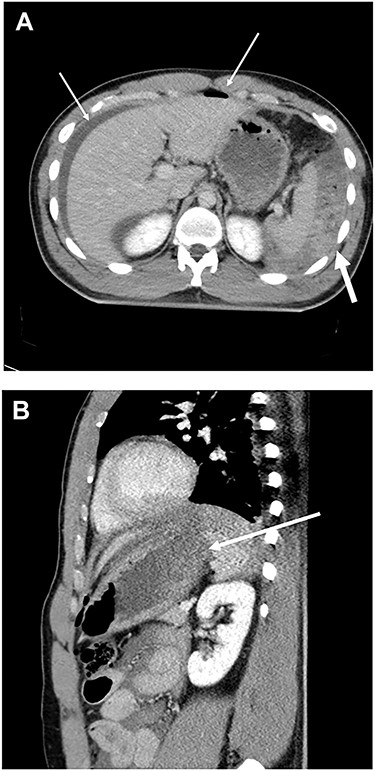
(A) CT scan of abdomen showed free air, ascites (thin arrow) and a large amount of food residue behind the spleen (thick arrow). (B) CT scan of abdomen showed disruption of gastric wall (arrow).
At laparotomy, blood ascites and a large amount of food residue were noted in the abdominal cavity. A burst was identified that resulted in a 10-cm hole that ran parallel to the long axis in a line from the cardia to the body of the anterior wall on the greater curvature (Fig. 3). There were no abnormalities to other abdominal organs.
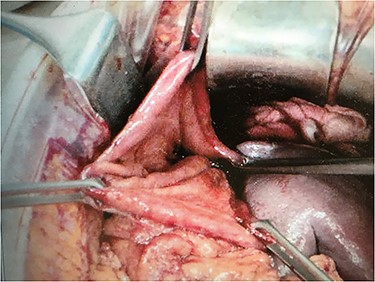
A burst hole of 10 cm was observed from the cardia to the body of the anterior wall at emergency laparotomy.
The food residue was carefully removed and the abdominal cavity was washed. Because the wound surface of the ruptured stump was clean, debridement was not necessary. A two-layer closure was performed with staples and Vicryls, and a drain was placed in the abdominal cavity.
The patient was administered 2-g ceftriaxone, intravenously for 10 days. A post-operative wound infection improved by drainage, and the patient was able to resume eating on the fourth day. The patient was eventually discharged on the 32nd day.
DISCUSSION
The first key paper describing blunt gastric rupture was published in 1975 by Yajko [1], who provided a detailed analysis of 35 cases from 1930 to 1973. Since then, results from investigations published over the past 30 years in the USA and Europe suggest that the frequency of gastric rupture ranges from 0.04 to 1.2% of all blunt abdominal traumas [2, 3], demonstrating that blunt gastric rupture seems to be a rare disease for emergency physicians.
In the present study, we examined 26 cases of gastric rupture due to blunt trauma that have occurred in Japan [4–6] (Table 1). We found that the average age was 40.1 years and that 22 of 26 cases were caused by traffic accidents. We classified the Japanese cases into the cardia, body and antrum areas, where the incidences were 24, 42 and 34%, respectively. In Japan, there is thus a tendency that fewer ruptures occur in the cardia and more occur in the antrum in comparison with those in Europe [7]. We then classified the ruptures according to the anterior wall, posterior wall, greater curvature and lesser curvature, and found that the incidences were 39, 7, 39 and 15%, respectively. In Japan, Europe and the USA [8], it seems that there is a tendency for rupture to occur in the anterior wall and the greater curvature.
Summary of 26 patients with blunt gastric rupture in Japan.
| Age (years) (n = 20) | 40.1 (5–76) | |
| Gender (n = 21) | Male/female | 17/4 |
| Causes (n = 26 | Traffic accident | 22 |
| Hit | 2 | |
| Fall | 2 | |
| Location (n = 21) | Cardia | 5 |
| Body | 11 | |
| Antrum | 9 | |
| (n = 26) | Anterior wall | 12 |
| Posterior wall | 2 | |
| Greater curvature | 11 | |
| Lesser curvature | 4 | |
| Number of site (n = 26) | Single | 21 |
| Multiple | 2 | |
| Transection | 3 | |
| Treatment (n = 26) | Simple closure | 19 |
| Gastrectomy | 6 | |
| Conservation | 1 | |
| Combined injury (n = 26) | No | 16 |
| Spleen | 4 | |
| Pancreas | 2 | |
| Intestine | 2 | |
| Spleen and liver | 1 | |
| Kidney | 1 | |
| Head | 1 | |
| Mortality (n = 26) | 0 |
When the stomach is distended from a recent meal, the pressure required for a rupture to occur is lower in the anterior wall and the greater curvature. Nanji [8] reported that 42% of all cases are postprandial. When a full stomach ruptures, a massive contamination distends the abdominal cavity. The most common complication after this event is an intra-abdominal abscess, which is often extensive, recurrent and very difficult to treat. The incidence of an intra-abdominal abscess is estimated to be up to 24% [9]. Considering these findings, contamination should be removed at laparotomy. Our case also sustained his injuries just 2 h after eating; consistently, a large amount of dyspeptic food was found in the abdominal cavity. Careful removal of the contamination took time and no abscess was found.
The damaged, ruptured stomach requires extensive surgical procedures for correction. Nineteen of twenty-one of the single rupture cases were treated with a simple closure, while six cases involving multiple rupture or transection required a gastrectomy.
Other organ injuries can frequently occur together with a gastric rupture, such as a splenic injury. Shinkawa [4] demonstrated that eight of nine patients with a gastric laceration had hepatic or pancreatic injuries, while no patients with a gastric rupture (n = 5) had such injury. This finding suggests that a distended stomach tends to rupture due to absorbing the impact; in this way, the stomach serves as an airbag, protecting the liver and pancreas. In our case, we also found no damage of other abdominal organs, which we propose is due to the large absorption of the compression forces by the fully dilated stomach. The large size of the ruptured hole (10 cm) supports this hypothesis. As for the rupture diameter, those exceeding 10 cm are very rare [3], with only seven reported cases [1, 8, 10].
An accurate diagnosis of a gastric rupture is often made during surgery. However, as in present case, careful evaluation of CT scan images is required to identify the disruption to the gastric wall or food residue outside the lumen. Furthermore, patient report of the injury occurring soon after eating might also help guide a pre-operative diagnosis.
CONCLUSION
Considering the rupture of a full stomach, careful removal of intra-abdominal contamination is essential for avoiding complications, such as infection. Most cases of single gastric rupture can be successfully managed by simple closure, but cases of multiple rupture or transection require a gastrectomy.

{kind=link}
{kind=link}
{kind=link}