





Abstract
Hepatic hydatid disease is located mainly in the right liver. It is usually solitary and asymptomatic; however, a large cyst may cause compression symptoms. We report a case of a huge echinococcal cyst located in segment IVb of the liver in a 39-year-old female, 17 x 11 cm in dimensions, causing persistent epigastric pain and discomfort. The diagnosis was made by a computed tomography (CT) scan, which showed the cystic mass with the characteristic daughter cysts and reactive caps (pericystic wall) consisting of fibrous connective tissue and calcifications. The patient underwent radical resection by total cysto-pericystectomy and had an uneventful postoperative course. Follow-up showed no recurrence in CT and normal liver function test. Total cysto-pericystectomy, as an alternative to hepatectomy, is the preferable choice of radical resection operation, nowadays, in the management of liver hydatid disease even in huge cysts.
INTRODUCTION
The incidence of liver echinococcal cyst or hepatic hydatid disease has considerably reduced across the world owing to concerted public health hygiene and sanitary measures to disrupt the parasite cycle between the main host (dog, wolf, fox) and the intermediate host (human, sheep, cow, pig). However, the condition is still endemic in some underdeveloped settings, while sporadic cases occur in the developed countries. Liver is the predominant location of the disease and the lesion is typically solitary. Surgery has remained the cornerstone of treatment despite the availability of more conservative treatment options [1–3].
Radical surgical management entailing complete resection of the intact cyst is the method of choice, although it requires considerable surgical dexterity and experience [4, 5]. The advances in operative techniques and availability of better energy sources have improved the feasibility of complete resection of even very large cysts. In contrast to hepatectomy, total cysto-pericystectomy or endocystectomy entails preservation of the liver parenchyma, while ensuring complete removal of the cystic lesion [6, 7].
In this paper, we present a challenging case of huge echinococcal cyst in liver segment IVb that was successfully managed by total cysto-pericystectomy. We summarize the experience gained and underline some critical aspects of the most demanding radical procedures for treatment of hepatic hydatid disease (total cysto-pericystectomy or hepatectomy).
CASE REPORT
Our patient was a 39-year-old female Syrian refugee who presented with compressive symptoms since one month, i.e. right abdominal and epigastric pain along with discomfort. On physical examination, a large mass with mild tenderness was palpable in the upper abdomen. Her past history was unremarkable. Her hematological and biochemical parameters (including liver function tests) were within the normal range. The definitive diagnosis was made based on computed tomography (CT) scan findings; it showed a cystic mass (size: 17 × 11 cm) containing the characteristic small daughter cysts and with clearly delineated reactive caps (pericystic wall) consisting of fibrous connective tissue and calcification (Fig. 1). Her American Society of Anesthesiologists (ASA) physical status score was ASA I.
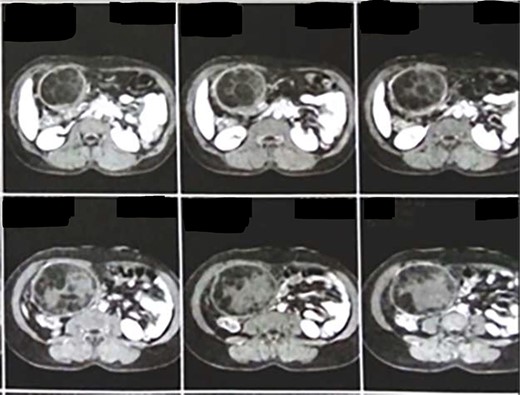
CT showing a cystic mass (size: 17 × 11 cm) containing the characteristic daughter cysts and with clearly delineated reactive caps (pericystic wall).
Surgery was performed via double Kocher incision (subcostal). Intraoperative examination revealed a cystic mass covered by great omentum and adhesions (Fig. 2). The operative field was packed with hypertonic saline gauze and compresses to isolate the lesion and prevent disease dissemination to other parts of the abdomen. Subsequently, liver mobilization was performed. Meticulous dissection was performed using the ultrasonic device Thunderbeat (Olympus America, USA) as the energy source. The cystic lesion (approximate diameter: 20 cm) originated from the segment IVb of the liver and was firmly adhered to the gall bladder. There was mild fibrosis of the gall bladder, however, it did not contain any gallstones. Both the cystic duct and the common bile duct were normal in diameter. Cholecystectomy was necessary for better access and mobilization of the cystic mass; the cystic mass was resected intact and completely along with the involved part of segment IVb liver (total closed cysto-pericystectomy). The removed intact specimen is shown in Figure 3. In addition, there was another small cyst (approximate diameter: 5 cm) in close proximity to the main cyst; it was removed completely by opening the cyst (endocystectomy). Intraoperative blood loss was minimal (<100 mL). Two closed drains were left in place prior to closure of the abdomen. Postoperatively, prophylactic antibiotics and albendazole were administered. The postoperative period was uneventful and the patient was discharged on the eighth postoperative day in good condition.
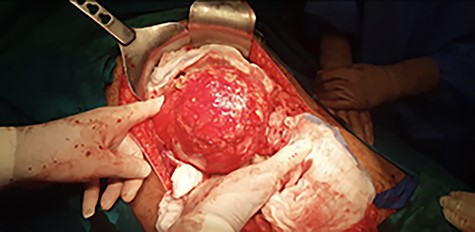
Intraoperative view showing the cystic mass covered by great omentum and adhesions.
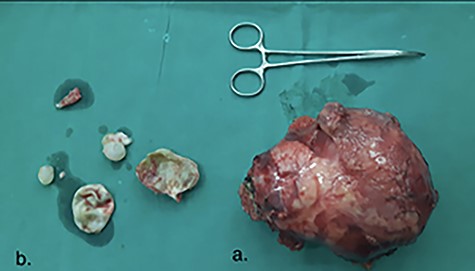
(a) The removed specimen, intact, showing the thickened outer or adventitia fibrous layer of hitine (huge cystic mass). (b) The small cyst, completely removed by opening it (endocystectomy); showing the outer cystic wall, two daughter cysts with hydatid debris material, and the inner laminated or germinal membrane.
The standard three-cycle treatment regimen of albendazole was prescribed (400 mg per oral twice daily for 28 days, followed by a gap of 14 days). Serum transaminase levels were monitored throughout the treatment.
At 1-year follow-up, there were no clinical or imaging signs of recurrence.
DISCUSSION
Various surgical techniques have been applied for the management of liver echinococcosis ranging from partial cystectomy to liver transplantation [4]. These include the most demanding radical procedures (total pericystectomy or hepatectomy) and the more conservative procedures (cyst evacuation, partial cystectomy, and drainage or omentoplasty) [5]. Complete removal of the cyst ensures permanent cure and should be the treatment of first-choice. Radical surgical procedures are well tolerated by patients and provide better results (low long-term recurrence rates) [7]. Total cysto-pericystectomy avoids the need for hepatic resection [8]. Subadventitial cystectomy should be considered as the standard surgical treatment in experienced hands, since it allows complete restoration of the operated liver [9].
Giant cysts (diameter ≥ 10 cm) are a surgical challenge requiring more caution, adequate experience and relevant instrumentation [8]. Our patient was young, fit (ASA score I) and had a symptomatic huge cyst in hepatic segment IVb. Total closed cysto-pericystectomy is the preferred choice in such cases and its excellent outcomes are well-documented [7, 8]. The second adjacent smaller cyst was managed by total open cysto-pericystectomy due to technical reasons. Therefore, postoperative prophylactic regimen of albendazole was considered necessary.
In the current era, minimally invasive surgery (i.e. laparoscopic or robotic approach) has been shown to be safe and effective approach even for radical liver resection or total cysto-pericystectomy, which can be either closed or open (the so-called subadventitial pericystectomy) [1, 4, 10].
In conclusion, total cysto-pericystectomy is currently the preferred choice for radical resection operation, and a viable alternative to hepatectomy, for the management of liver hydatid disease, even in patients with huge cysts. The more conservative partial cystectomy and drainage procedure or omentoplasty should be avoided in such cases.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}