





Abstract
We report herein a 14-month-old boy with a left-sided peeping testis. At the age of 1 month, the left testis was palpated between the inguinal canal and the scrotum. When he was 6 months old, ultrasonography showed the left testis in the inguinal canal. At the age of 13 months, the left testis was not palpable. At the age of 14 months, he underwent surgery for a planned inguinal orchidopexy with a preoperative diagnosis of an undescended testis. When the inguinal canal was opened, a patent processus vaginalis was observed and the testis was found inside the abdominal cavity. The patent processus vaginalis was closed, a dartos pouch was created and the testis was guided into the pouch and fixed to its wall. We describe a case of a peeping testis moving from the inguinal position into the abdomen.
INTRODUCTION
An undescended testis (cryptorchidism) remains in the abdomen or the groin instead of descending into the scrotum. Retractile testes descend into the scrotum but can easily move back into the inguinal canal as a reflex response to stimulation. Peeping testes are nonpalpable and are able to move from the abdomen into the inguinal canal with the application of intra-abdominal pressure [1].
CASE REPORT
A14-month-old boy was admitted to our hospital to undergo inguinal orchidopexy. At the age of 1 month, the left testis was palpable between the inguinal canal and the scrotum. When he was 6 months old, ultrasonography showed the left testis inside the inguinal canal (Fig. 1). At the age of 13 months, the patient was seen in the outpatient clinic for preoperative examination in preparation for inguinal orchidopexy; the left testis was not palpable at that time. At the age of 14 months, we began surgery with a preoperative diagnosis of an undescended testis. When the inguinal canal was opened, only a patent processus vaginalis was visible (Fig. 2). After incision of the membrane, we were able to retrieve the testis from the abdominal cavity (Fig. 3a). The patent processus vaginalis was closed, a dartos pouch was created and the testis was guided into the pouch and fixed to its wall (Fig. 3b).
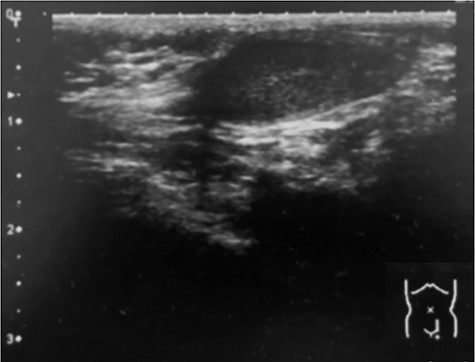
Ultrasonography (6 months of age). The left testis is located within the inguinal canal.
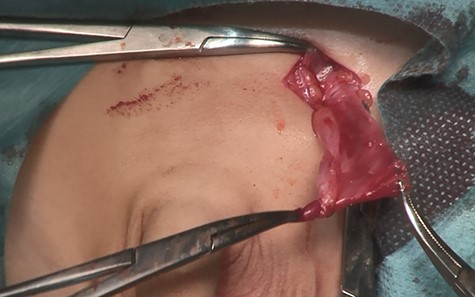
Intraoperative photography (14 months of age). After opening the inguinal canal, only a patent processus vaginalis is visible.
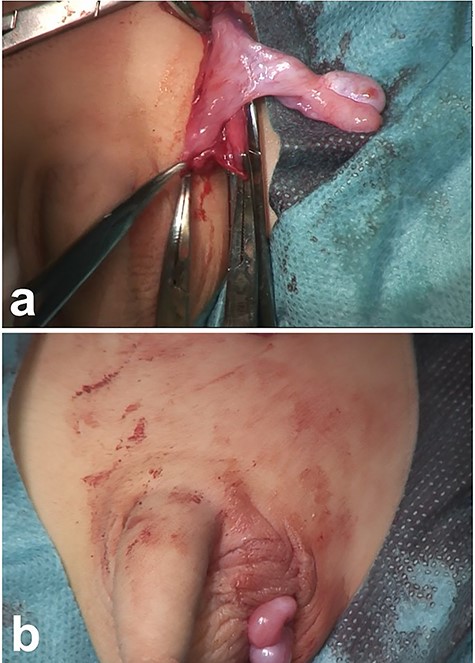
Intraoperative photography (14 months of age). (a) The testis is retrieved from the abdominal cavity. (b) After the patent processus vaginalis is closed, the testis is guided into a dartos pouch and fixed to the pouch wall.
DISCUSSION
This case report describes a patient with peeping testis that was not suspected prior to surgery. Between October 2015 and October 2019, we operated on 72 patients with retractile testes and 56 patients with undescended testes. Of the patients with undescended testes, two developed an intra-abdominal testis and one had a peeping testis. In the 72 patients with retractile testes, 47 underwent trans-scrotal orchidopexy and 25 underwent inguinal orchidopexy. The 56 patients with true undescended testes underwent inguinal orchidopexy, and the two patients with intra-abdominal testes underwent 2-stage Fowler–Stephens orchidopexy. Of 128 patients with nonpalpable testes in the scrotum, only a single patient at our institution had a peeping testis.
Current guidelines recommend that orchidopexy for undescended testis should be undertaken before 2 years of age because of the risk for torsion, infertility and malignant transformation [1]. The incidence of torsion in undescended testes is thought to be higher than in scrotal testes [2–6]. The literature describing torsion of an undescended testicle is mostly limited to case reports [7–8]. In the largest case series concerning testicular torsion in the inguinal canal, the mean patient age was 29.15 ± 20.21 months, a higher age than the usual recommended age for treatment [8]. Torsion inside the inguinal canal is associated with the presence of an inguinal hernia [9]. In a report describing the long-term outcome of patients with retractile testis, 14.1% developed an undescended testis or experienced a decrease in testicular size requiring orchidopexy. The risk of these complications is higher in patients diagnosed at a younger age (1.3 ± 0.9 years) [10].
Peeping testes are primarily located in the intra-abdominal position, descending into the inguinal canal with application of intra-abdominal pressure. Peeping testis is usually associated with the presence of an inguinal hernia; it returns to its original intra-abdominal position by pressing on the inguinal region externally [1]. In our patient, the testis moved spontaneously from the inguinal position to the intra-abdominal position. Patients with undescended testicles associated with inguinal hernias have a risk for torsion and should undergo repair by 2 years of age. Regular ultrasonography is useful to investigate the location of the testis and the existence of an inguinal hernia.
Author Disclosure Statement
No competing financial interests or funding exists in connection with this manuscript.
Conflict of interest statement
None declared.

{kind=link}
{kind=link}
{kind=link}