





Abstract
Angioleiomyomas are defined as benign dermal or subcutaneous tumours consisting of smooth muscle cells arranged around vascular channels. Head and neck angioleiomyomas are rarely encountered as they usually occur in the extremities. We report a case of a 71-year-old male, who presented with a 3-month history of a painless lateral neck lump. Ultrasound and computed tomography scans localised the suspicious hypervascular tumour to the right supraclavicular fossa between the two heads of sternocleidomastoid muscle. He subsequently underwent an excisional biopsy, where histological analysis determined that the lateral neck mass was a venous subtype angioleiomyoma. To the best of our knowledge, this is only the third reported case of an angioleiomyoma in the supraclavicular fossa. Although supraclavicular masses are typically synonymous with malignancy, this case report highlights that angioleiomyoma should be considered as a differential diagnosis when investigating patients with a lateral neck lump.
INTRODUCTION
Leiomyomas are benign smooth muscle-derived tumours, of which there are four types: leiomyoma, angioleiomyoma, epithelioid leiomyoma and mesectodermal leiomyoma [1]. Angioleiomyoma (vascular leiomyoma) is defined by the World Health Organisation as a benign dermal or subcutaneous tumour comprised of well-differentiated smooth muscle cells arranged around multiple vascular channels [2]. Angioleiomyomas are classified into three subtypes based on their histological architecture:
Solid—tightly compacted smooth muscle cells positioned in variably intersecting bundles between slit-like vascular channels.
Venous—variably sized venous lumina with thick muscular walls blending with loose intervascular smooth muscle bundles.
Cavernous—multiple dilated vascular channels with either thick or thin walls between limited numbers of smooth muscle bundles [1–3].
Angioleiomyomas are most common in patients between 40 and 60 years of age and usually present as a firm, small, slow-growing mass [2]. Cavernous and venous subtype angioleiomyomas are more prevalent in males than females, while the reverse is true for the solid subtype [4]. Patients often complain of a painful lump, which can be exacerbated by exposure to cold or wind, or by pregnancy, pressure or menses [2]. Interestingly, solid subtype angioleiomyomas are more likely to cause pain but venous subtype tumours are typically painless [4]. Approximately 4–5% of all benign soft tissue tumours are found to be angioleiomyomas [2]. Of these, 89% are localised to the extremities, especially below the knee [5]. Angioleiomyomas in the head and neck region are rarely seen and account for only 8.5% of all angioleiomyomas [5].
CASE REPORT
A 71-year-old male presented with a 3-month history of a painless lateral neck lump. It would become more prominent when he performed a Valsalva manoeuvre. He had no lumps elsewhere on his body and was otherwise asymptomatic with no significant past medical history.
On examination, there was a 20-mm non-pulsatile, non-tender, solid, subcutaneous mass in the right supraclavicular fossa between the two heads of sternocleidomastoid muscle (SCM). It was mobile and not adherent to the overlying skin. There were no skin changes and no lymphadenopathy.
Routine blood tests showed no abnormalities and his tumour markers were normal. A neck ultrasound demonstrated a heterogeneous solid mass with marked internal vascularity located within the base of the right neck (Fig. 1). It was closely associated with SCM but remained external to the carotid and visceral space. A computed tomography (CT) scan of the neck concurred with the ultrasound findings, suggestive of a suspicious well-circumscribed hypervascular mass within the right supraclavicular fossa at the origin of SCM (Fig. 2).
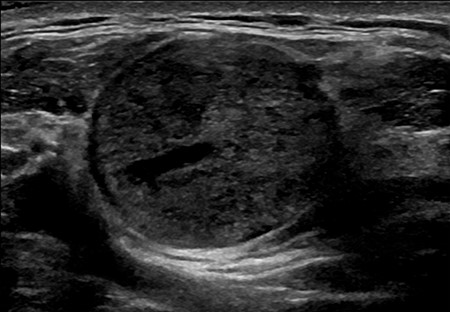
An ultrasound image of the well-circumscribed 22 × 22 × 25 mm round solid mass, which is located within the right supraclavicular fossa and intimately associated with the sternocleidomastoid muscle at its origin. The lesion demonstrates marked internal vascularity and is superficial to the carotid and visceral space.
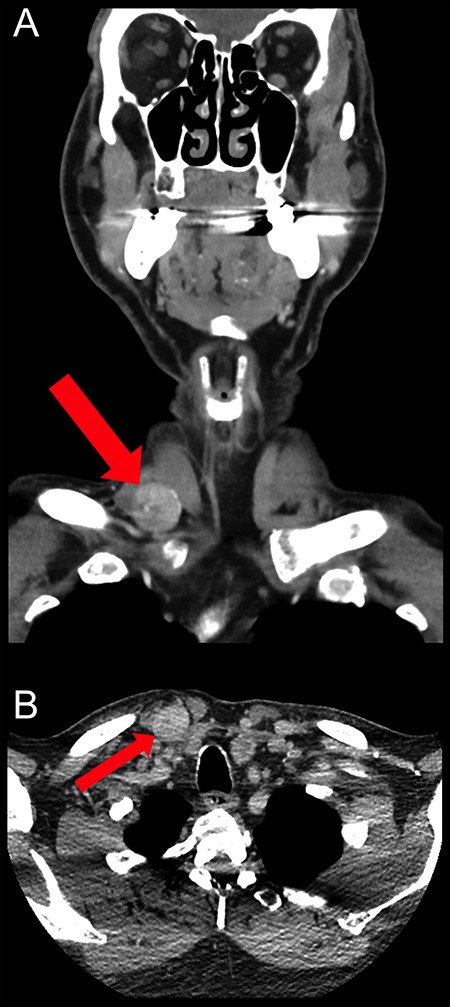
Coronal (A) and axial (B) CT scan images showing the well-circumscribed hypervascular mass measuring 22 × 19 mm within the right supraclavicular fossa at the origin of sternocleidomastoid muscle. It lies outside the carotid and visceral space with no underlying erosion of the clavicle.
Because of its hypervascularity, the neck tumour was deemed not amenable to ultrasound-guided biopsy. Hence, the patient subsequently underwent an excisional biopsy, where the operative findings were that of a vascular-rich mass superior to the medial end of the clavicle and wedged between the two heads of SCM. Histopathological analysis determined that the mass was composed of thick-walled blood vessels with prominent muscle (Fig. 3). There was focal myxoid degenerative change and focal chondroid metaplasia with no evidence of malignancy, suggestive of an angioleiomyoma. The patient was reviewed 3 months post-operatively and was recovering well.
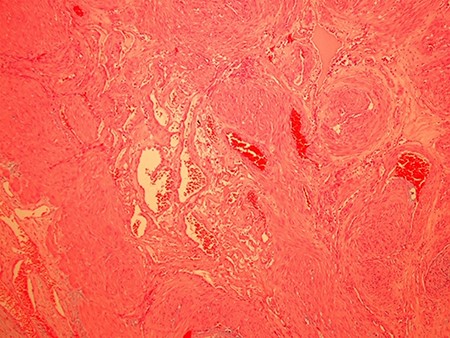
A representative haematoxylin and eosin (H&E) histological image (100× magnification) of the right supraclavicular venous subtype angioleiomyoma showing variably sized blood vessels with thick walls and prominent muscle.
DISCUSSION
Currently, there are <200 cases described in the literature of angioleiomyomas occurring within various locations in the head and neck [5]. Here, we report only the third documented case of an angioleiomyoma within a specific part of the lateral neck space—the supraclavicular fossa. The other two reported cases of supraclavicular angioleiomyomas were detailed in two different retrospective studies on head and neck angioleiomyomas, which are described below.
The first retrospective study reported a deep supraclavicular angioleiomyoma in an asymptomatic 23-year-old male [6]. The patient had a CT scan and subsequently a fine needle aspirate (FNA), which was non-diagnostic [6]. An excisional biopsy was performed, where histological analysis demonstrated a venous subtype angioleiomyoma with associated hyaline change [6]. It has been suggested that FNA and cytology are of no benefit in the diagnosis of head and neck angioleiomyomas and may lead to misdiagnosis [5].
The second retrospective study described an asymptomatic 55-year-old male with an angioleiomyoma in the deep supraclavicular space [7]. The patient had an ultrasound followed by an excisional biopsy, where histological analysis showed a solid subtype angioleiomyoma [7]. Unlike our case, our patient’s angioleiomyoma was of the venous subtype with associated myxoid and chondroid changes. Morimoto suggested that myxoid changes were common in venous subtype angioleiomyomas, and that both myxoid and hyaline changes were rarely present in painful tumours [3, 4].
The pre-operative diagnosis of angioleiomyomas in the head and neck is challenging [5]. In our case, it was thought that the supraclavicular mass was ectopic thyroid. Indeed, the presence of a supraclavicular mass is usually concerning for malignancy, with differential diagnoses including lymphoma and malignant lymphadenopathy [8]. The diagnosis is further complicated because imaging characteristics of angioleiomyomas are shared with those of other tumours and hence do not offer an accurate pre-operative diagnosis [5, 9, 10]. Albeit some form of imaging modality would be beneficial to assist with pre-operative planning. The best method for diagnosis and treatment of head and neck angioleiomyomas is histological examination via complete surgical resection [5, 7, 10].
In conclusion, we present a rare case of a venous subtype angioleiomyoma in the supraclavicular fossa. This case report raises questions as to the best pre-operative imaging modality for the diagnosis of neck lumps. It also highlights that angioleiomyoma should be considered as a differential diagnosis when investigating patients with a lateral neck lump.
DISCLOSURE STATEMENT
This is a statement that declares that no financial support or relationships exist that may pose a conflict of interest by disclosing at the time of submission any financial arrangements they have with a company whose product figures prominently in the submitted manuscript or with a company making a competing product.

{kind=link}
{kind=link}
{kind=link}