





Abstract
Sinonasal undifferentiated carcinoma (SNUC) is a rare tumor with poor prognosis and high incidence of distant metastasis, even when a good loco-regional control is achieved.
We report the case of a 43-year-old female with SNUC diagnosis. Craniofacial resection with orbital exenteration and radiotherapy in tumor bed and lymph node chain was performed. After 10 months, SNUC hepatic relapse (sIII and sVIII) is diagnosed. We administered chemotherapy and then, surgical resection was carried out. After surgery, two new relapses were diagnosed, at 9 and 21 months where surgical management was performed in both cases. 56 months after SNUC diagnosis, the patient has no evidence of recurrence.
Recommended oncological clinical guidelines for distant metastases in SNUC are chemotherapy. Surgical management in oligometastatic disease in SNUC should be considered.
INTRODUCTION
Sinonasal undifferentiated carcinoma (SNUC) is a rare, poorly differentiated type of tumor, with rapid progression and high risk of distant metastasis with an incidence of 0.02/100 000. It is more frequent in men under 45 years of age [1]. This type of tumor, which was first described in 1986, is associated with poor prognosis [2] and distant metastasis even when a loco-regional control is achieved. It presents high rates of local recurrence [3].
Surgery combined with chemoradiotherapy has shown lower relapse rate than surgery alone or surgery combined with radiotherapy [4, 5] Distant metastasis rate in patients under surveillance is about 25% [5].
Nowadays, there are no prospective randomized trials to guide therapy. The main evidence comes from small retrospective single institution series in highly specialized centers. Thus, it is important to report the results obtained in case reports to improve the overall results of the treatment of these patients, particularly in the treatment of SNUC distant metastasis.
CASE REPORT
We report the case of a 43-year-old female within 6 months of rhinorrhea. At presentation, a mass that reached the entire right nasal fossa was observed. A fiberoptic bronchoscopy with biopsies was performed and an undifferentiated carcinoma with negative neuroendocrine markers was diagnosed (High-weight cytokeratins, p63 and p16 determination were positive, which are correlated with the human papillomavirus).
Paranasal sinuses CT showed a solid lesion located in middle, upper and common right meatus, ethmoid hemibody, with extension to lamina papyracea and lamina cribosa with superior oblique infiltration. (Fig. 1)
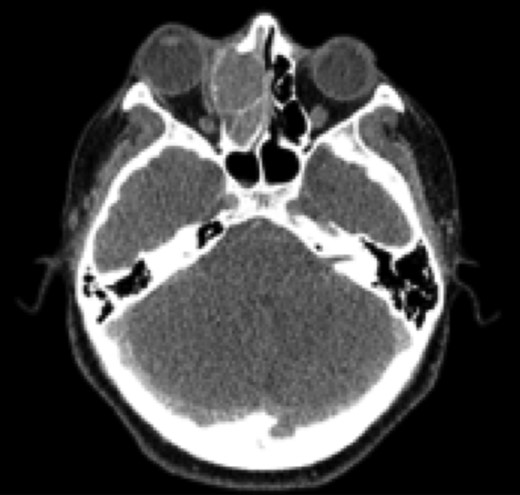
Pre-operative CT scan. SNUC.
Surgical procedure was performed with right craniofacial resection and orbital exenteration. Treatment was completed with radiotherapy (50 Gy on a tumor bed and 60 Gy on a ganglionic chain) for one month.
Ten months later, CT revealed two hepatic lesions (segment III of 3 cm and segment VII of 1 cm) (Fig. 2) The biopsy confirmed the original histology of SNUC. Chemotherapy with docetaxel 75 mg/m2, cisplatin 75 mg/m2 and 5 FU 750 mg/m2 every 3 weeks for 3 months was administrated. Because of minimal response was achieved after chemotherapy (Fig. 2) a non-anatomical metastasectomy was performed.
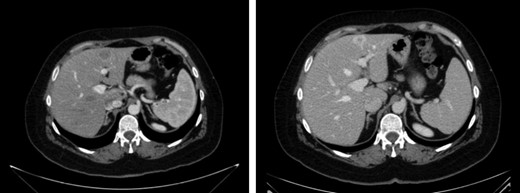
CT scan first relapse. Liver metastases: sIII and sVII 2.2 CT scan after neoadjuvant chemotherapy.
A new hepatic node in segment VII was observed nine months later (Fig. 3). Systemic treatment was administrated with cisplatin (75 mg/m2) and cetuximab for three months. At the end of the treatment, another non-anatomical metastasectomy with free margins was performed.
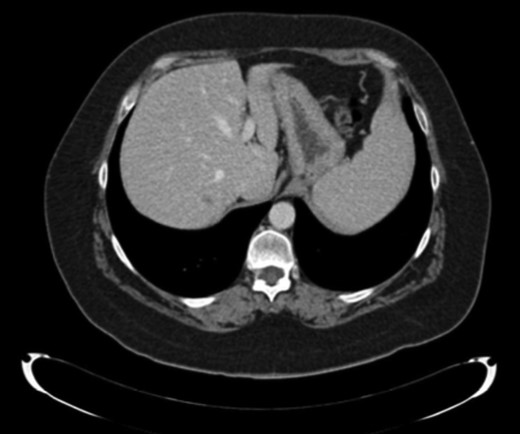
CT scan. Liver metastases sVII.
Finally, 12 months after this second liver surgery, a new hepatic lesion in left hepatic lobe of 3 cm was identified (Fig. 4). Systemic treatment was re-initiated with Cisplatin (75 mg/m2) and Cetuximab for 2 months. After that, left hepatectomy was performed with tumor-free surgical margins without subsequent complications. Surgical specimen revealed undifferentiated tumor.
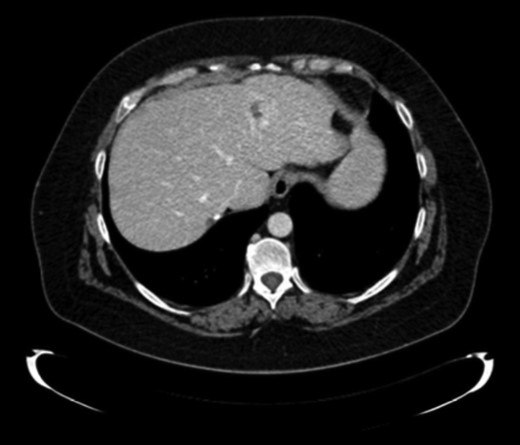
Liver metastases LHL.
With a follow-up of 56 months after diagnosis and 1 year after the last surgery, patient has no evidence of recurrence.
DISCUSSION
SNUC is a rare and aggressive malignancy with a rapid clinical progression and an overall poor prognosis. SNUC should always be included in the differential diagnosis of paranasal tumor [6, 7], because most of these tumors are squamous cell [8].
Risk factors related to poor prognosis and distant metastases are location, size and positive lymph nodes. SNUC has the poorest prognosis of head and neck tumors, with a 5-year overall survival around 40%. Moreover, ethmoidal location has poorer prognosis than those of the nasal cavity or maxillary sinus. When paranasal tumors develop distant metastasis (4%), 1 year overall survival decreases to 20% with a median survival of 6 months. Loco-regional relapses are about 51%, with a 5-years overall survival of 20% [7].
Nowadays, recommended oncological clinical guidelines for distant metastases in SNUC are chemotherapy, with platinum-based regimens [9]. The only evidence in surgical treatment of oligometastatic disease in SNUC is based in case reports or short series of cases [10]. However, surgical treatment of distant metastases in SNUC is rarely included in clinical guidelines.
The importance of this case report is that with and aggressive surgical and systemic treatment approach we have achieved a complete response of this poor prognosis tumor with an overall survival of 56 months.
We believe that patients with SNUC tumors with oligometastatic disease, controlled disease and absence of progression to chemotherapy are good candidates for surgical resection.
To end-up and although there are no well-designed studies to demonstrate this oncological benefit of surgical resection, we consider that every surgical procedures performed beyond the clinical guidelines should be reported, in order to improve clinical evidence and provide to patients the best available treatment, particularly in cancer.
Conflict of Interest statement
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}