





Abstract
Metastases to the hand and wrist are extremely rare, with <250 cases described in the literature. We present a case of acrometastasis of colon adenocarcinoma to the scaphoid in an 81-year-old male. Adenocarcinoma of the colon metastasizes to bone in an estimated 10% of cases; however, we are unaware of reports of this tumor metastasizing to the scaphoid or to any of the other carpal bones. We were able to identify only two cases of scaphoid metastases in the literature. This case highlights the potential for metastatic disease and other lesions to develop in the scaphoid and carpus.
INTRODUCTION
Metastasis to the hand and wrist, or acrometastasis, rarely occurs. Of all osseous metastatic lesions, the incidence of distal limb metastasis is ~0.1% [1]. Nearly 250 cases of hand and wrist metastases have been described in the literature, with fairly consistent epidemiological findings presented across series and reviews [1–5]. The distal phalanx was the most common site of upper extremity acrometastasis, while carpal bone involvement was exceptional. Of the reported acrometastases, the most common primary neoplasm was lung, followed by renal and breast.
Colon adenocarcinoma with metastasis to bone occurs in only 10% of patients. The majority of these osseous lesions appear in the vertebral column. Metastasis to the hand and wrist has been reported in 0.007–0.2% of patients with adenocarcinoma of the colon [6]. A literature search of MEDLINE/PubMed revealed two cases of metastases to the scaphoid [7, 8]. No reports were found of metastatic colon adenocarcinoma discovered in the carpal bones, or specifically, the scaphoid. Here we present the case of a patient with history of colon adenocarcinoma and wrist pain that was determined to be metastasis to the scaphoid. This case study was approved by our local Institutional Review Board and granted a HIPAA waiver of consent.
CASE REPORT
An 81-year-old male presented with complaints of right wrist pain. He had injured his wrist 6 months prior while changing a wheel bearing. Since that time, he complained of worsening right wrist pain that was located radially and exacerbated with activity. He had begun experiencing paresthesia of his right fingertips, but denied any constitutional symptoms.
His past medical history was significant for colon adenocarcinoma, for which he underwent total colectomy and ileostomy nearly one year prior to presentation. He had finished a chemotherapy regimen, and a recent PET scan was negative for thoracic and abdominal metastasis.
Physical exam revealed no palpable masses and no erythema or swelling. There was tenderness to palpation in the anatomic snuffbox. Radial deviation and extension of the wrist caused an increase in pain. Sensation was intact in the median, radial and ulnar nerve distributions. Anterior interosseous, posterior interosseous and ulnar nerve motor function was intact. Distal pulses were normal.
Radiographs of the right hand and wrist revealed a lytic lesion in the scaphoid with nearly complete destruction of the distal pole (Fig. 1a–c). The lateral radiograph also demonstrated some abnormal scalloping of the distal radius articular surface (Fig. 1c). Magnetic resonance imaging (MRI) showed destructive changes of the radial sided carpus (Fig. 2a and b), suggestive of neoplastic or infectious processes, but was inconclusive.
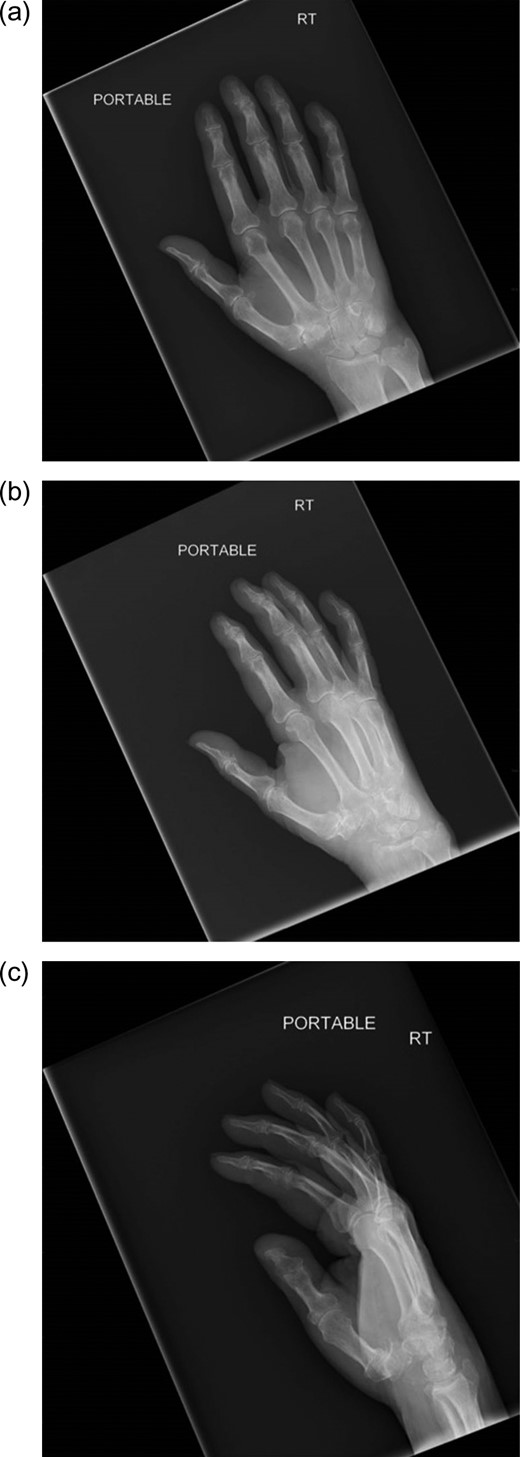
(a) AP image of the wrist showing a destructive lesion within the carpus. (b) Oblique image of the wrist showing a destructive lesion within the carpus. (c) Lateral view of the wrist showing a destructive lesion within the scaphoid. Note the near dissolution of the distal scaphoid and scalloping of the distal radius articular surface.
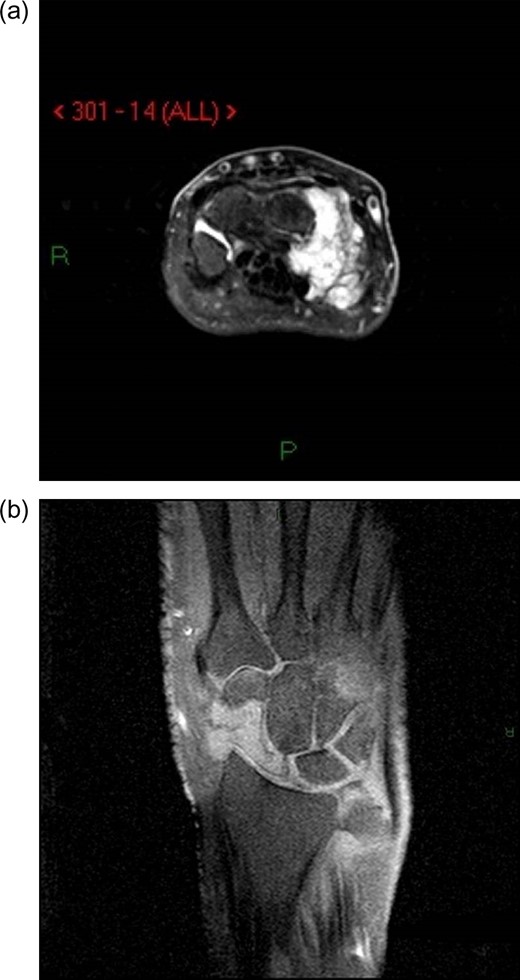
(a) Axillary MRI of the wrist. (b) Coronal MRI of the wrist.
After a thorough discussion with the patient, we decided to perform a proximal row carpectomy (PRC) along with biopsy and culture of the lesion. The PRC was performed through a dorsal approach. Once the carpus was exposed, a gelatinous mass was seen emanating from the scaphoid (Fig. 3). The mass was eroding into the lunate, trapezium and distal radius articular surface. The entirety of the gelatinous mass was excised and sent for biopsy (Fig. 4). Culture was also taken at this time. The remainder of the scaphoid, as well as the lunate and triquetrum were excised, thus completing the PRC. Copious irrigation was then performed followed by a layered closure.

Gelatinous lesion emanating from the scaphoid and cavernous defect in the scaphoid.

Tumor excised from scaphoid.
Pathology revealed glandular tissue consistent with metastatic adenocarcinoma of the colon. Cultures were negative.
During routine postoperative follow-up, his physical exam revealed improved pain with a decreased range of motion at the wrist. He was evaluated by his medical oncologist after surgery and another course of chemotherapy was given. Radiation treatment was discussed, but the patient declined secondary to the ongoing pain relief he experienced after surgery. The patient survived 1 year after his scaphoid metastases were discovered.
DISCUSSION
Metastatic disease should be suspected in patients with destructive lesions of the carpus, metacarpals and phalanges. These lesions, which can be found incidentally or after prolonged wrist or hand pain, may be misdiagnosed as degenerative changes or other skeletal diseases [1–9]. The lack of recognition or misdiagnosis can lead to delay in care or improper treatment [3]. A review of 221 cases of wrist and hand metastases found that 30% of these metastases represented the first manifestation of the occult malignancy [4]. Our report highlights the importance of considering the possibility of scaphoid metastases from all primary sources, including colon adenocarcinoma [9, 10].
Distant spread of malignant cells from the primary location is believed to occur mostly by hematogenous pathways. It has been postulated that the distal phalanx is the most commonly involved area of the hand due to its susceptibility to trauma and increased blood flow [3, 4]. There have been other reported cases of metastatic spread to exact locations of direct hand trauma possibly as a result of the increased blood flow, prostaglandin production, and other factors contributing to cell attachment and migration [4, 5, 9, 10]. Our patient had a similar episode of trauma to his wrist shortly before his lesion appeared.
There is currently no treatment standard for acrometastases, as the prognosis relates to the characteristics and behavior of the primary tumor. Acrometastasis generally portends a poor prognosis, with an average survival of 6 months after discovery of the lesion(s) [3]. Therefore, treatment of metastatic cancer to the hand or wrist is typically palliative—directed toward analgesia and preservation of hand and wrist function. Treatment should consist of surgery for symptom relief, followed by chemotherapy for control of tumor burden. Hypofractionated radiation therapy may also be used for palliative treatment with good results [3, 5]. Our implementation of PRC for pain relief and local control is a novel technique not described in the literature for symptomatic treatment of carpal, specifically scaphoid, metastases.
In conclusion, metastatic disease should be suspected in patients with a destructive bone lesion in the wrist or hand and a history of cancer. Metastases to the hand may also be the first sign of disease. In this report, the PRC provided excellent pain relief with good local control. This case describes metastatic adenocarcinoma located in the scaphoid, which has not been described in the literature to date.
Acknowledgements
The authors thank Caitlynn K. Smith, BS for her assistance with this report.
Conflict of Interest statement
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}