





Abstract
Metastases of colorectal carcinoma (CRC) in the testis are very rare and indicate an advanced stage of disease. In this case report, we present a patient with adenocarcinoma in the sigmoid colon with metastasis in the right testis. Testicular metastasis of CRC is mostly diagnosed late because of their low incidence rate. Patients with CRC and testicular metastasis have a poor prognosis. In this case, the patient turned out to have peritoneal metastasis and one should be aware that testicular metastasis could be the first sign of widespread disease.
INTRODUCTION
Colorectal carcinoma (CRC) is the third most common diagnosed cancer and the fourth most common cause of cancer-related death globally. In the Netherlands, the incident rate is 77.2 per 100 000 people per year [1]. The median age at diagnosis is approximately 70 years in developed countries [2]. CRC generally metastasizes to liver, lungs, bones, brain and spinal cord. Metastases to the testis are rare and less common than metastases to the ovary (Krukenberg tumor). The cornerstone of therapy for testicular metastases encompasses orchiectomy and chemotherapy. We present a case of a male patient with cancer in the sigmoid colon with metastases to both liver and testis to show that CRC can also metastasize to the testis and can be the first presentation of peritoneal metastasis.
CASE REPORT
A 75-year-old Caucasian man was referred to the hospital for rectal blood loss. There were no other symptoms. Medical history showed no signs of fever and hematemesis. The patient had no history of gastrointestinal diseases. His prior medical history only showed hypertension and poliomyelitis. No known relatives had CRC, endometrial-, ovarian-, gastric- or urethral cancer or inflammatory bowel disease.
At physical examination, he had a pyknic build and was afebrile. He had a scar on the lower left abdomen due to surgery as a child for cauda equina syndrome due to poliomyelitis. His abdomen was not distended, nor were there any masses felt. On rectal examination, no stenosis or nodule was felt.
Laboratory test showed a hemoglobin of 13.7 g/dL, leukocytes of 5.8 × 109/L, thrombocytes of 173 billion/L and a carcinoembryonic antigen (CEA) of 3.2 ng/mL.
Colonoscopy revealed a polyp in the sigmoid colon and an obstructing tumor suspected for CRC (20 cm from the anal verge) (Fig. 1). An abdominal contrast-enhanced computed tomography showed four lesions in the liver suspected for metastases without lymphadenopathy (Fig. 2). Magnetic resonance of the liver showed five lesions suspected for metastases. Chest X-ray was normal.

Colonoscopy of the sigmoid colon revealing a polyp suspected for malignancy.
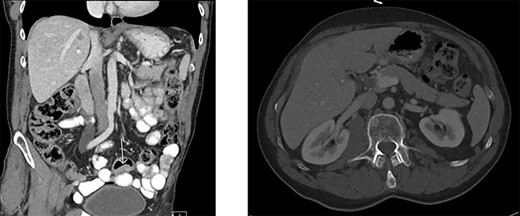
Abdominal contrast-enhanced computed tomography. A. Tumor in the sigmoid colon. B. Four hypodense lesions in liver suspected for metastases.
A laparoscopic resection of the sigmoid colon with a loop colostomy was performed. Also a right hemihepatectomy with additional radio frequent ablation (RFA) of one lesion was executed. Pathologic analyses revealed an adenocarcinoma of the sigmoid colon with a maximum diameter of four centimeters. The tumor was radically removed and no positive lymph nodes were found. Pathological classification was pT4N0M1 (TNM 8th edition AJCC). No adjuvant chemotherapy was given according to national guidelines.
As part of follow-up 6 months after resection, laboratory tests for CEA, an ultrasound of the liver and a colonoscopy were performed. Postoperative CEA was 4.0 ng/mL. Ultrasound of the liver showed post-therapeutic changes after RFA and surgery. No metastases were found (Fig. 3). With colonoscopy, one polyp was found in the caecum. A punch biopsy was performed and revealed an adenoma with low-grade dysplasia.
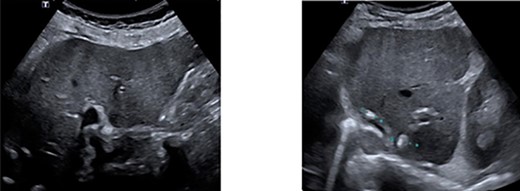
Ultrasonography of the liver showing no progression of disease. A. Right lobe. B. Left lobe.
One year after surgery, his right testis was swollen and painful. There was no dysuria or hematuria. On scrotal examination, a small nodule (approximately 1 cm in diameter) was felt in his right testis. Ultrasonography showed a hydrocele of the right testis with thickening of the scrotal wall and a tumorous mass (Fig. 4). An orchiectomy was performed and pathologic analyses revealed a metastasis of the adenocarcinoma between tunica albuginea and tunica vaginalis. He started palliative chemotherapy containing capecitabine and bevacizumab. The CT scan after three cycles of chemotherapy showed a partial remission.
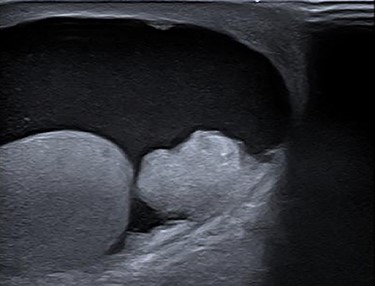
Ultrasonography of right testis showing hydrocele and a tumorous mass.
DISCUSSION
CRC is the most frequent cancer of the digestive tract. With an incidence of 77.2 per 100 000 per year in the Netherlands, it is the third most common tumor [1].
No single risk factor accounts for most cases of CRC. Risk factors that have been identified in epidemiological studies for developing CRC are the following: age, male sex, family history of CRC or inflammatory bowel disease, excessive alcohol intake, smoking, obesity and diabetes [3, 4].
Symptoms of CRC are rectal blood loss, melena, abdominal pain, obstruction, mucus in the stool, altered bowel habits or a false sense of urgency. CRC generally metastasizes to the lymph nodes, liver and lung, Metastases in the testis are rare, although some cases have been reported [5, 6].
Excluding lymphoma and leukemia, common tumors that metastasize to the testis are prostate (35%), lung (20%), malignant melanoma (10%) and kidney (8%) [7]. Testicular metastases of CRC are rare; in the last 30 years, only seventeen cases have been described. In a recent case series of 26 patients with testicular metastases, the primary tumor was not found in 62% of the cases. Furthermore, almost all testicular metastases are unilateral [6].
The exact mechanism of testicular metastasizing remains unknown. Several theories have been suggested, including retrograde lymphatic extension, retrograde venous extension, arterial embolization and direct tumor invasion [8].
Complete curation of testicular metastases in colorectal cancer is not possible. However, debulking of the testicular mass with adjuvant chemotherapy can be executed to achieve best overall survival. Chemotherapy alone will not be as effective since the testes are considered a sanctuary site for chemotherapy [9].
Prognosis depends mainly on the presence of other metastases and also on radicality of resection and recurrence of peritoneal dissemination. With a median survival rate of 9.1 months after diagnosis, prognosis remains poor [10]. In this case, testicular metastasis turned out to be the first sign of peritoneal metastasis.
CONCLUSION
Testicular metastases in CRC are rare, and pathogenesis still remains unclear. It tends to occur in late stage of disease and has a poor prognosis. Testicular metastases can be a first sign of peritoneal metastasis and one should be aware that it can indicate widespread disease.
Conflict of Interest STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}