





Abstract
The traumatic hearing loss is a common finding after head trauma that involves the temporal bone fracture or skull base injury, but the late presentation of the hearing loss bilaterally is a rare presentation. This case report describes the rare and late presentation of bilateral conductive hearing loss 1-year after the head trauma, limited to ossicular chain disruption and hearing loss. This case of post head trauma that was limited to ossicular chain distribution progressed to bilateral conductive hearing loss without temporal bone fracture. A 14-year-old male was presented conductive hearing loss of one year after head injury, CT scan revealed bilateral ossicles disruption. Afterwards, osicuoloplasty was performed which improved the hearing of the patient. In conclusion, bilateral hearing loss with no obvious skull fracture should be suspected and investigated so an early intervention could be established. The CT was considered the imaging modality of choice for ossicular chain distribution.
INTRODUCTION
Traumatic head injury (THI) is any trauma that causes abnormality of normal brain function either by minor or severe disruption of that function (1). The THI is responsible for 2.5 million emergency cases in the USA in 2013 causing ~56 000 deaths (1). One of the outcomes is hearing loss as it occurs in THI especially after temporal bone injuries or fracture base of the skull (2). The transverse type of temporal fracture was associated with sensorineural hearing loss (3), while the conductive type was associated with damage of the petrous pyramid and middle ear structure (2). However, there are reported cases of hearing loss without apparent skull fracture. Labyrinthine concussion or direct damage to central auditory pathway are possible causes of this type of hearing loss (2). Studies found that it may be caused by haemorrhage inside the ear canal, microscopic injuries to the brainstem or injuries to vestibulocochlear nerve (2, 4). A systematic review found that the incidence of the hearing loss without skull fracture ranges from 0.9% to 58%. The study suggested that the hearing loss is considered a common sequalae of the traumatic brain injury (5).
CASE REPORT
A 14-year-old male patient presented to the ENT clinic with bilateral hearing loss with no other otolaryngological symptoms. History from the patient stated a road traffic accident (RTA) 12 months ago. Meanwhile, the patient had no hearing problems prior to the RTA. Furthermore, detailed history of the accident revealed that the patient had no apparent skull injuries while pure tone audiometry (PTA) on presentation revealed bilateral conductive hearing loss and auditory brainstem response revealed right mild hearing loss and left moderate hearing loss. As a result, he was fitted with hearing aid for four months after presentation and was not compliant to it on the long-term. The patient is a non-smoker and is medically free with normal developmental milestones and negative family history of hearing complaints. Local examination of the ear revealed intact but minimally retracted tympanic membrane bilaterally. PTA was done in 2014 revealed right mild to moderate mixed hearing loss and conductive hearing loss at low frequency (Table 1). Meanwhile, the left ear had mild to moderate sensory hearing loss at high frequency (Table 2). The speech audiogram results show equal canal volume in both ears, less tympanometry pressure on the right ear and less compliance on the right ear (Table 3). The CT showed that both ossicular chains are deranged, and bilateral abnormal ossicles with no fracture or mass (Figures 1–3).
The speech audiogram (pre-op) and was done in 2014: Audiogram of the Right ear
| 250 | 500 | 1k | 2k | 3k | 4k | 8k | |
|---|---|---|---|---|---|---|---|
| BC | 10 | 10 | 15 | 15 | |||
| AC | 40 | 40 | 40 | 45 | 50 |
Audiogram of the Left ear
| 250 | 500 | 1k | 2k | 3k | 4k | 8k | |
|---|---|---|---|---|---|---|---|
| BC | 10 | 30 | |||||
| AC | 60 | 50 | 55 | 45 | 50 | 60 |
Speech Audiogram
| The speech audiogram results | |
|---|---|
| Canal volume | |
| Right | 1,2 |
| Left | 1,2 |
| Tympanometry pressure | |
| Right | −35 |
| Left | −7 |
| Compliance | |
| Right | −2,54 |
| Left | −1,76 |
| Type | RT:B |
| Lt: C | |
The speech audiogram Post-op in 2018.
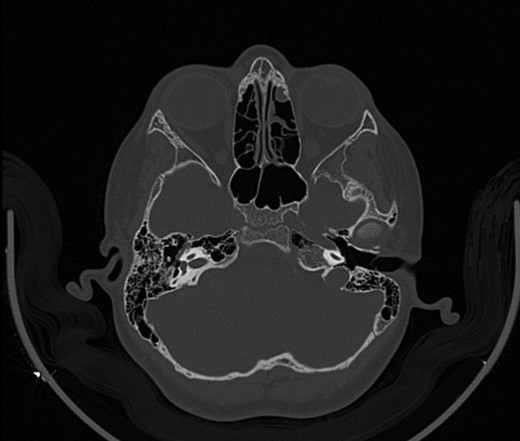
CT mastoid, deranged right side ossicular disruption.
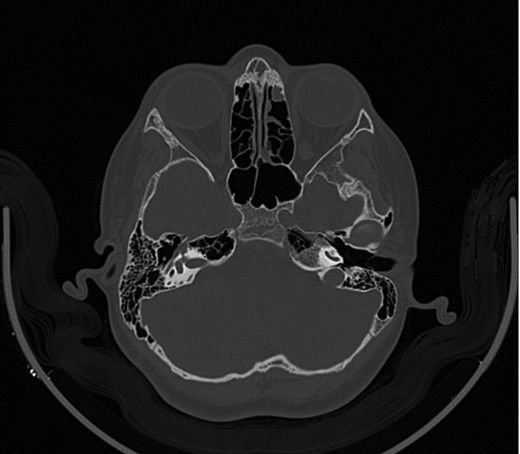
CT mastoid, deranged right side ossicular disruption.
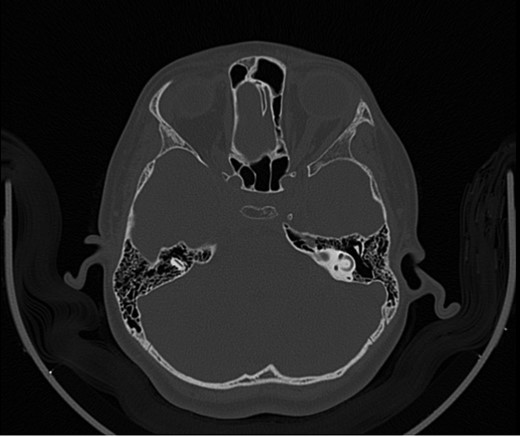
CT mastoid, deranged left side ossicular disruption.
The patient underwent ossiculoplasty in 2014. However, four years later in 2018, right ossiculoplasty, intraoperative finding revealed right intact tympanic membrane, stapes in place with normal movement, the incus was rotated and displaced while the malleus was displaced anteriorly. It was repaired by removing the incus and inserted the PROP and supported by cartilage. After the surgery, the patient improved substantially bilaterally according to the PTA (Tables 4 and 5).
Audiogram of the RT ear
| 250 | 500 | 1k | 2k | 3k | 4k | 8k | |
|---|---|---|---|---|---|---|---|
| BC | 10 | −10 | 10 | 35 | |||
| AC | 40 | 40 | 45 | 55 | 70 | 75 | 70 |
Audiogram of the Lt ear
| 250 | 500 | 1k | 2k | 3k | 4k | 8k | |
|---|---|---|---|---|---|---|---|
| BC | 10 | 5 | 0 | 0 | 5 | ||
| AC | 5 | 15 | 10 | 5 | 10 | 55 |
DISCUSSION
In this case report, the initial findings indicate bilateral traumatic conductive hearing loss. However, there were no evidence of temporal bone fracture or base skull fracture were evident. Before the surgery, the patient had both conductive and sensorineural hearing loss on the left side which was treated by left osicuoloplasty. Moreover, persistent hearing loss after the history of trauma on both sides was evident during the follow-up during the 4-years leading to surgery.
Previous studies reported that hearing loss without head injury was due to brainstem injury or temporal lobe lesions. The most common cause of traumatic hearing loss was fall from height followed by RTAs as the case in our case report (5, 6). The long-sustained hearing loss after accidents was also reported by Belgmalam et al. who followed the patients for 7–11 years and found that 36% of patients had persistent hearing loss (6), while Podoshin et al. found that 18% of traumatic hearing loss patients had improved after six months (7). However, correlation between cognitive functions with the auditory functions was positive which meant that brain injury without evident skull fracture was associated with the hearing loss (2, 6). Lastly, barotrauma injury is common in the absence of temporal bone fracture making it the most probable cause of the hearing loss in this case. In a study by Powers et al., barotrauma was evident by accompanying pressure waves to the head injury which spreads to the intracerebral structures (8). These waves caused Superior semicircular canal dehiscence which resulted in audiologic and auditory symptoms (9). In barotrauma of the middle ear, exudate and signs of inflammation,such as blood congestion and bleeding, results in hearing loss with progressive ossicular disruption (10).
The diagnostic modality for the THI was imaging techniques. A study found that CT was the imaging of choice for head trauma cases while MRI was used as imaging modalities for such underlying cause (5, 6). Based on a systematic review, the CT was the best imaging modalities for conductive hearing loss while MRI was the best for sensorineural hearing loss (6).
The traumatic hearing loss in TBI patients was accompanied with other symptoms including vertigo, tinnitus and hyperacusis (5). However, in this patient, it was only hearing loss which is considered the most common complaint.
In our case, the surgical treatment had a positive outcome on the patient. In the literature, the similar case reports treated the patients medically with steroids with no need of surgery. However, other studies tried steroids for hearing loss and no significant improvement was found. Therefore, surgical intervention of such cases must be considered.
ACKNOWLEDGEMENTS
We would like to thank the support it had from the research committee of Ohud Hospital in providing us with the necessary tools and access to make this report, we would like to also thank the patient and his family for giving us the approval of publishing this report.
CONFLICT OF INTEREST STATEMENT
None.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}