





Abstract
Cystic lymphangiomas are rare benign tumours and their actual incidence in the colon is unclear. Within the large bowel, these lesions are often submucosal and are incidental findings on colonoscopy.
A 43-year-old man with colonic lymphangioma presented with a 7-month history of abdominal pain and altered bowel habits. Computed tomography showed a cystic mass lesion at the distal descending colon. Colonoscopy revealed a smooth, polypoid mass, initially thought as an inverting diverticulum. He underwent laparoscopic high anterior resection. The pathological analysis revealed the descending colon mass to be a lymphangioma with no evidence of diverticulosis.
There is increasing incidence in lymphangioma due to the increasing accessibility to colonoscopy, particularly for asymptomatic or subacute disease. Although colonoscopic excision, sclerotherapy and use of steroids or fibrin glue have been advocated as possible modes of treatment, surgical excision is still considered to be the treatment of choice.
INTRODUCTION
Lymphangioma is a neoplasm of lymph vessels that commonly occur in children and appear in the head, neck and axilla [1, 2]. They are uncommon in the colon and presentations of this disease are limited to case reports in the literature [3]. Within the large bowel, these lesions are often submucosal and are often incidental findings on colonoscopy [3]. The most common presentations include cystic rupture, bleeding or pain. Rarely do they cause intestinal obstruction and there are only six reported cases of lymphangioma causing intussusception [4–9]. Furthermore, colonic lymphangioma is more readily reported in patients from an East Asian background and most reported cases are from Japan, Korea and Taiwan [3, 6].
We present a case of subacute intussusception secondary to a colonic lymphangioma in a Caucasian patient.
CASE PRESENTATION
A 43-year-old man presented with seven months of intermittent lower abdominal pain and altered bowel habit. The patient denied having similar symptoms in the past or any history of abdominal surgery. He had no past medical history or familial history of colorectal malignancy. On presentation, he appears well with no tenderness or palpable masses on abdominal examination. A computed tomography of the abdomen and pelvis demonstrated a 13 × 10 × 10 mm3 ovoid lesion in the distal descending colon and no evidence obstruction and associated regional lymphadenopathy (Fig. 1). A colonoscopy performed confirmed the ovoid mass, for which an inverted diverticulum was initially suspected (Fig. 2). Mucosal biopsies did not demonstrate any pathological changes. The patient underwent laparoscopic high anterior resection with an uncomplicated post-operative course and a rapid recovery.
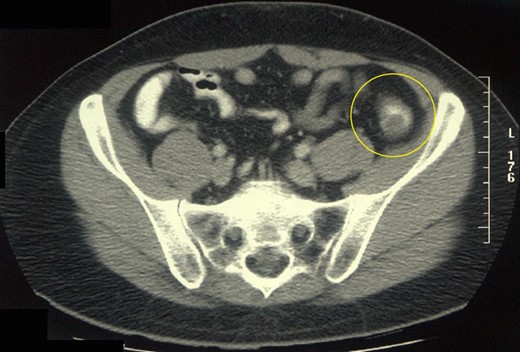
Abdominal CT scan of the patient showing a space-occupying lesion in the distal descending colon.
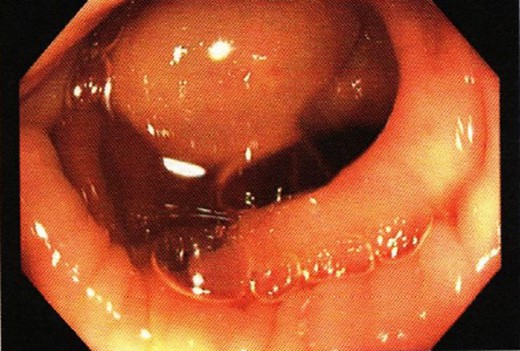
Colonoscopic finding showing a smooth distal descending colon tumour.
The intussuscepting mass was completely excised with clear margins (Fig. 3). Histopathology showed a unilocular cyst in the submucosa with a thin fibrous wall lined by a monolayer of lymphatic endothelium confirmed with immunohistochemistry for D2 40 (podoplanin) consistent with a lymphangioma. Some smaller lymphatic channels were noted in the cyst wall. No evidence of diverticulosis was identified (Fig. 4).
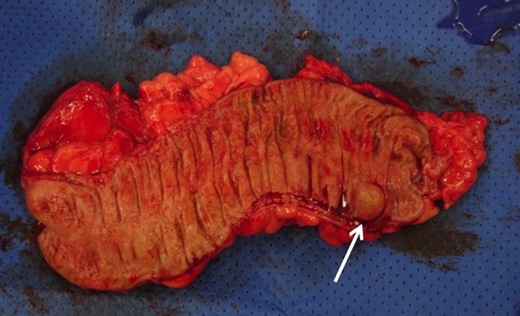
Gross picture of the high anterior resection specimen showing the descending colon lymphangioma.
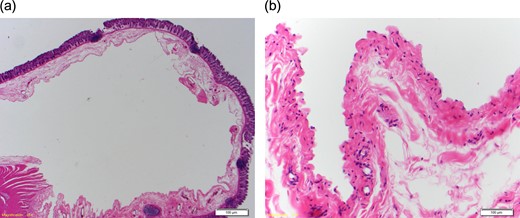
Haematoxylin and eosin stained section ((a) low power magnification, (b) high power magnification) showing a unilocular cyst in the submucosa lined by lymphatic endothelium with a thin fibrous wall containing occasional bundles of smooth muscle. Some smaller adjacent lymphatic channels are noted at high power.
DISCUSSION
This is the first reported case of descending colon lymphangioma presenting as an intussusception in a Caucasian patient. At present, there are only six previous case reports of colonic lymphangioma presenting with intussusception [4–9]. Almost all cases were in East Asian patients and had cystic lymphangioma in the caecum. Also, unlike previous cases, which reported an acute hospital admission and emergency surgery, this patient underwent an elective laparoscopic high anterior resection.
Lymphangiomas can occur anywhere and in any age group. These benign tumours are very uncommon in the abdomen, and intra-abdominal lymphangiomas more frequently present in the small bowel mesentery and are mostly asymptomatic in adults [1]. Symptomatic intra-abdominal lymphangiomas may present over months to years if no acute obstruction occurs and diagnosis is often difficult [1]. In recent years, there is increasing incidence in lymphangioma due to the increasing accessibility to colonoscopy, particularly for asymptomatic disease [3].
Although colonoscopic excision, sclerotherapy and use of steroids or fibrin glue have been advocated as possible modes of treatment, surgical excision is still considered to be the treatment of choice [10]. Malignant transformation of colonic lymphangiomas does not occur. However, these lesions can still be complicated by concurrent adenoma or malignancy. Also, the potential to grow and subsequently cause obstruction or invade adjacent structures can possibly lead to life-threatening complications. Moreover, removal of the entire lesion as completely as possible is recognized as the most important factor for reducing the risk of recurrence [10].
CONFLICT OF INTEREST STATEMENT
The authors declare no potential financial or non-financial conflicts of interest with respect to the research, authorship and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship and/or publication of this article. Informed consent was obtained from the participant included in the study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}