





Abstract
Intracranial teratomas are rare. We report a case of a purely monodermal teratoma manifesting as intracranial growing teratoma syndrome. To the best of our knowledge, this is the first report of such nature in the literature.
INTRODUCTION
Intracranial germ cell tumours (IGCTs) are a rare, heterogenous group of lesions, which most frequently arise in the pineal and suprasellar regions [1]. IGCT can be classified as germinomas, non-germinomatous germ cell tumours (NGGCTs) and teratomas. Teratomas constitute a group of NGGCTs that comprises of different tissue’s types recapitulating development from the three embryonic germ layers. Intracranial teratomas have a predilection for midline structures and can be classified into mature teratomas, immature teratomas and teratomas with malignant transformation [2].
The term growing teratoma syndrome (GTS) was first described by Logothetis [3] for extracranial germ cell tumours that demonstrated paradoxical growth of solely mature teratomatous elements despite normalization of tumour markers.
We describe a presumptive case of intracranial GTS (iGTS), notable for its occurrence in an adult, the long interval following the completion of treatment (consisting of radiation therapy alone) to development, and the purely monodermal character of the mature teratomatous mass.
CASE REPORT
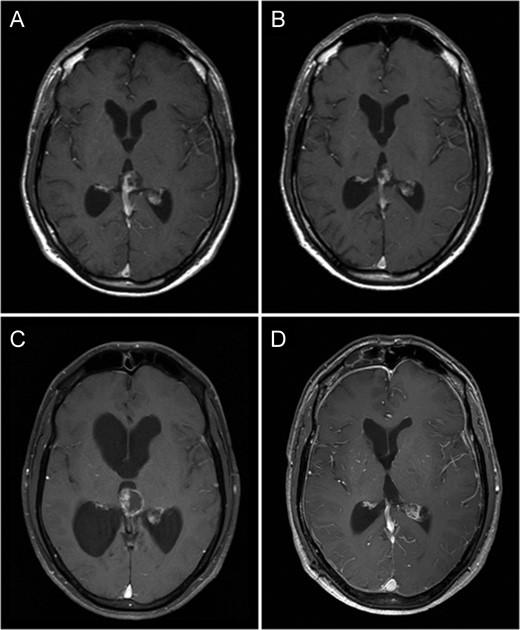
Fat saturated axial gadolinium enhanced T1 weighted MR Brain Image Series (A—July 2000, B—October 2003, C—July 2009 and D—November 2010). Image A demonstrates a heterogeneously enhancing lesion involving the pineal gland with enhancing solid as well as cystic components. Image B demonstrates a reduction in size of this lesion following radiation therapy. Image C demonstrates a prominent increase in the cystic component of the lesion associated with obstructive hydrocephalus. Image D demonstrates no residual tumour or contrast enhancement 1-year following surgery.
The patient received 50 Gy/28 fractions of whole brain radiation therapy, which corresponded with reduction in size of the mass. He made an excellent recovery with complete resolution of his symptoms. He was kept under radiological surveillance for a period of 5 years with no signs of progression (Fig. 1B).
Nine years after his initial presentation, the patient represented with worsening headache, staggering gait and mild memory impairment. Imaging revealed an increase in size of the pineal mass, with a marked enlargement of the cystic component, associated with extension into the third ventricle and obstructive hydrocephalus (Fig. 1 C).
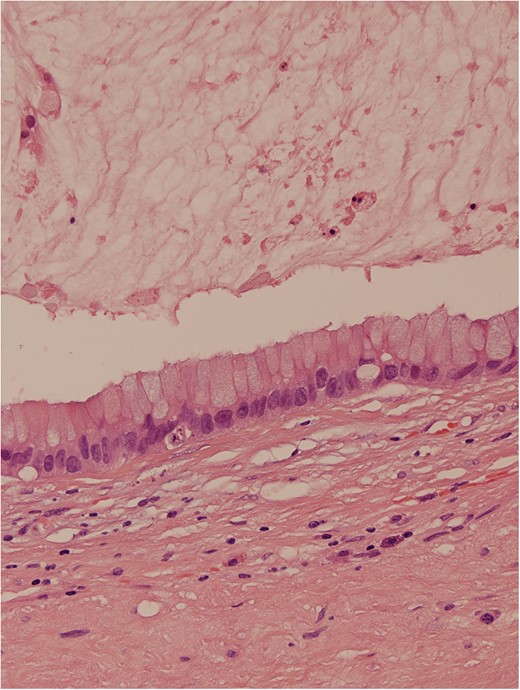
Haematoxylin and eosin stain demonstrated a mucin-containing cyst, lined by a partly detached columnar epithelium containing numerous goblet cells, surrounded by a dense, lightly inflamed fibrous stroma and a thin rind of calcified tissue probably representing residual pineal gland. The epithelium lining the cyst comprised cuboidal and columnar epithelial cells largely arranged as a monolayer, but with focal stratification, mild cytologic atypia and rare mitoses, but no malignant change. The cyst contained copious mucin, with an inflammatory and histiocytic reaction. Dystrophic calcification was present, both within the cyst and in the dense fibrous wall. Immediately peripheral to the main central cyst, there were a few smaller outpouchings into the stroma lined by epithelium of similar nature. No other germ cell elements were identified. The features were interpreted to represent mature cystic teratoma with only a monodermal tissue element (mucinous, cystic glandular element), with no other neoplastic germ cell component, most probably of pineal origin.
DISCUSSION
GTS is defined by the development of an enlarging mass of mature teratomatous tissue, during or after adjuvant therapy for a germ cell tumour (GCT), associated with normalization of tumour markers. No GCT component other than mature teratoma forms the mass. A literature search revealed seven isolated case reports of iGTS; however, a recent retrospective analysis of two Korean centres claimed a total incidence of 11 cases out of 170 patients with IGCT [4].
Although histopathological diagnosis of the pineal mass was not established at the very first presentation, we believe on clinicoradiological grounds, that the original pineal mass was an iGCT, and hence this represents a genuine example of iGTS. We hypothesize, using clinicoradiological correlation, the initial diagnosis would favour that of a mixed germ cell tumour with germinomatous as well as teratomatous components. The imaging at presentation revealed a heterogeneously enhancing predominantly solid lesion with some cystic components—this would be inconsistent with a benign mucinous (e.g. enteric) cyst, and hence the enlarging residual mass cannot simply represent an enlarging recurrence of a simple neuro-enteric or related cyst. MR spectroscopy was unavailable for further evaluation of the tumour.
To the best of our knowledge, this is the first case of iGTS in which the mature teratomatous mass was purely monodermal in character. Additionally, we could find only one previous case of iGTS following radiation therapy alone [5].
The role of radiotherapy in causing GTS has yet to be established. In this case, it is difficult to establish whether the growth of the tumour was related to radiotherapy or just very unusual natural progression of the teratoma. As the tumour did initially respond to radiation, this would favour the former.
The pathogenesis of GTS is unclear. It is possible that therapy induces transformation from immature teratoma to mature teratomatous tissue, or, alternatively, destroys all immature components leaving only residual mature teratoma. Although it is well recognized that treated pineal mixed germ cell neoplasms may result in residual teratoma [6], and although pure teratomas are known to grow, rapid enlargement is extremely unusual in the absence of malignant transformation [5]. The process which mediates the acquisition of marked proliferative activity in GTS cells is unclear, although it is possible that cystic enlargement of the epithelial component may have produced the GTS.
This report emphasizes the importance of histological diagnosis prior to commencing treatment and illustrates the need for long-term follow-up in iGCT management. When an enlarging mass develops following treatment for IGCT, GTS must be distinguished from tumour recurrence. Pathological confirmation is recommended, particularly if there are discordant imaging and tumour marker findings.
CONFLICT OF INTEREST STATEMENT
The authors have no personal, financial or institutional interest in any of the drugs, material or devices described in this article.

{kind=link}
{kind=link}