





Abstract
The association between elbow dislocation, medial epicondyle fracture with intra-articular fragment entrapment and ulnar neuropraxia is very unfrequent with only a few cases reported in the literature, the mechanism of injury of the ulnar nerve is still unknown. This injury requires surgical management with stable fixation of the medial epicondyle fragment to allow early range of motion, the choice whether or not to perform an ulnar decompression and nerve transposition remains a controversy between orthopedic surgeons. We present the case of a 14-year-old patient that suffered an elbow dislocation with intra-articular entrapment of the medial epicondyle and ulnar neuropraxia that was managed with open reduction and fixation of the medial epicondyle with good functional outcomes.
INTRODUCTION
Elbow dislocations are a rare finding between children; they are account for 3–6% of all elbow injuries [1]. Medial epicondyle fractures consist of 12% of all elbow fractures [2]. Intra-articular entrapment of the fragment occurs in 5–18% of the cases of fractures of the medial epicondyle [3]. The association between pediatric elbow dislocation, intra-articular entrapment of the medial epicondyle and ulnar nerve injury is very unfrequent with only a few cases reported in the literature, mostly in a delayed presentation [4–6] In a case series of 14 cases over a period of 14 years, the only associated nerve damage to a case of elbow dislocation and intra-articular entrapment of the medial epicondyle fragment was median nerve entrapment syndrome, in one patient [2, 4, 5] The functional outcomes of similar injuries are variable and are highly related to the time after which the ulnar injury was detected.
CASE REPORT
A 14-year-old male patient presented to the emergencies department complaining of intense pain in the left elbow secondary to a fall with an outstretched hand while practicing soccer. He had no significant comorbidities. At physical examination he presented with deformity located on the left elbow, he was unable to passively or actively mobilize it, he reported paresthesias and diminished sensation located on the fifth and fourth digit. X-rays showed a dislocation on the left elbow and an avulsive fracture of the medial epicondyle of the distal humerus (Fig. 1). He was taken to the operating room where a closed manipulation was performed; however the reduction was not achieved due to the interposition of the fractured medial epicondyle. A medial approach to the elbow was performed; intra-operative findings included rupture of the medial capsule and intra-articular interposition of the fragment of the medial epicondyle with a posterolateral dislocation of the elbow, the ulnar nerve showed compressive injuries at the site of the fracture (Fig. 2). Extraction and fixation of the interposed intra-articular fragment was performed followed by elbow reduction and a medial capsule repair, without ulnar nerve transposition (Fig. 3). The patient was left with a posterior splint for a month. After a 3 month follow-up, he has recovered full range of motion of the elbow with recovery of strength and sensation over the distribution of the ulnar nerve.
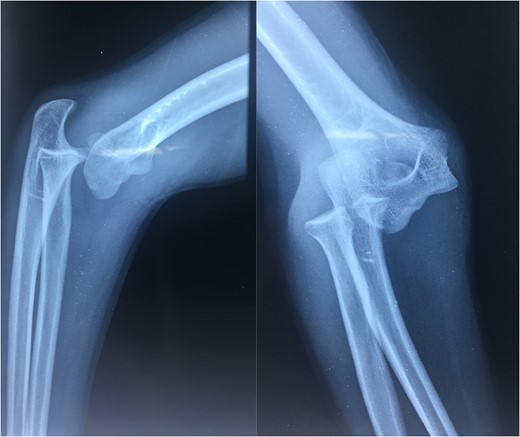
X-rays showing an initial view of the patients left elbow.
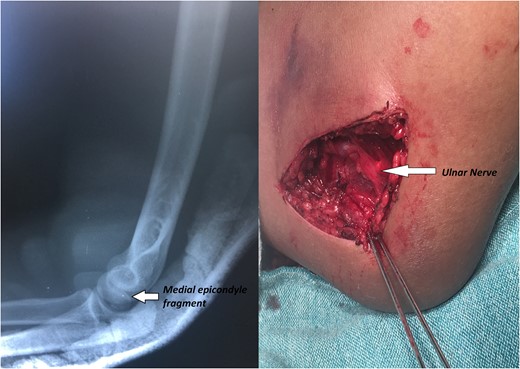
X-rays showing the result of the first attempt of closed manipulation and open reduction.

Post-operative radiographs.
DISCUSSION
Pediatric traumatic elbow dislocations are rare injuries; most commonly they are encountered as complex dislocations in a posterolateral direction, and are more frequently associated to fractures of the medial epicondyle [1, 7] The finding of an ulnar injury associated to traumatic elbow dislocation and incarceration of the fragment of a medial epicondyle fracture is uncommon, the mechanism of the ulnar injury is still debated; Lima (2013) stated that the injury was produced due to direct compression of the ulnar nerve from the fracture fragment or to elbow joint manipulation, Raymond (2010) attributed the ulnar injury to the vulnerability of the nerve as it enters the soft tissues between the heads of the flexor carpi ulnaris in its trajectory, associated to significant soft tissue injury to the roof of the cubital tunnel leaving the nerve exposed at the time of fracture fixation [5, 8].
It is of common agreement that the management of a pediatric elbow dislocation associated to medial epicondyle with fragment entrapment requires stable fixation since elbow stiffness is the most common complication following medial epicondyle fractures [6, 9].
We decided to fix the fragment with k-wires taking in account of the frequent complications of the use of screws, such as the need of hardware removal in almost 20% of patients of the larger case series revised, however the use of screws has been recommended, especially in cases with older patients, mainly to gain stability and allow early range of motion [3, 7–9].
There is no general agreement in the literature whether or not to perform an ulnar decompression and transposition. In this case, we considered that the ulnar neuropraxia was produced by the pressure of the bony structures of the elbow over the nerve and considered that the injury would resolve after reduction and fracture fixation. Disadvantages associated to ulnar decompression and transposition include: larger incision and operative time, higher risk of neuritis due to implant irritation [6, 10].
CONCLUSION
Bone dislocations associated to intra-articular entrapment of a medial epicondyle fracture are rare injuries that must be managed surgically. The mechanism of injury of the ulnar nerve is still undefined. There is no general agreement whether to perform or not a ulnar decompression and transposition, but good functional outcomes can be achieved without these in selected cases.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}