Abstract
Laparoscopic surgery through a single incision is gaining popularity with different stakeholders. The advantages of improved cosmetics, decreased postoperative pain and blood loss continue to attract patients from different surgical fields. Multidisciplinary approach to different surgical entities through a single incision has just been introduced. We report the first case of a synchronous single-port access (SPA) laparoscopic right hemicolectomy and laparoscopic-assisted vaginal hysterectomy with bilateral salpingo-oophorectomy through a single incision above the umbilicus in a 48-year-old female with ascending colon mass and uterine mass with good postoperative outcomes. SPA laparoscopic surgery is feasible for multidisciplinary approach in resectable tumors.
INTRODUCTION
The first recorded synchronous laparoscopic surgery was in Zurich, Switzerland last 2006 where Breitenstein et al. used the vagina to remove the sigmoid colon and uterus [1]. Similarly, transvaginal extraction of the spleen and uterus was done in a community hospital in Arizona, USA last 2013 [2]. Meanwhile, Fistarol et al. from Brazil used a single trocar access port through the umbilicus for an adnexal mass excision and cholecystectomy in 2014 [3]. This case report hopes to shift paradigms encouraging multidisciplinary approach through minimally invasive surgery in a single incision port.
CASE REPORT
This is a case of a 48-year-old female clerk with 3 months of fatigue getting worse with occasional diarrhea. There was no exertional dyspnea, dizziness, loss of consciousness, rectal bleeding and abdominal pain. Past medical history includes well-controlled Diabetes Mellitus Type 2. Previous surgeries include bilateral tubal ligation. Patient is a nonsmoker and occasional alcoholic drinker. Last Pap smear and mammogram were normal. She is G3P3(3003) with menopause at 46 years old. Family history includes ovarian cancer and hypertension on maternal side.
Physical examination reveals body mass index of 31.8 kg/m2, pallor, without abdominal masses or tenderness. Pelvic exam showed parous introitus, atrophy of vaginal mucosa, multiparous cervix, 10-week size uterus, no adnexal masses or tenderness, no discharges.
On initial evaluation, she was transfused 2 units of packed red blood cells due to hemoglobin of 6 g/dl. Other pertinent laboratory findings include carcinoembryonic antigen 6.6 mg/ml, calcium 10.4 mg/dl and fasting blood sugar 202 mg/dl. Colonoscopy done showed an ascending colon mass in the hepatic flexure and a rectal polyp. Biopsy revealed fragments of infiltrating moderately differentiated adenocarcinoma and benign hyperplastic polyp, respectively.
Computerized axial tomography scan of the abdomen revealed wall thickening or mass involving the proximal ascending colon with multiple subcentimeter lymph nodes within mesentery adjacent to this portion (Fig.
1). There was no evidence of metastatic disease. A 3.8 × 3.3 cm hypodense mass located in the central portion of the uterus was also noted (Fig.
2).

Figure 1:
CT scan of abdomen showing ascending colon mass.
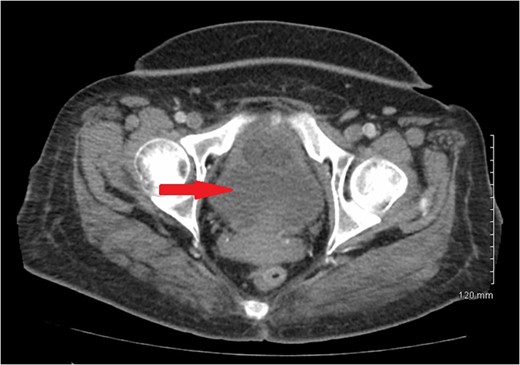
Figure 2:
CT scan of pelvis showing uterine hypodense mass.
A vertical 2 cm incision was made above the umbilicus to facilitate extraction of the mass. A commercial transumbilical single-port access (SPA) was placed (Fig.
3). The ileum, cecum and right colon were mobilized from its retroperitoneal attachments. The omentum was then dissected off the transverse colon, and hepatic flexure was subsequently taken down. Next, the right branch of the middle colic artery and the ileocolic pedicle was isolated and doubly ligated with the laparoscopic blunt tip vessel sealer and divider. Laparoscopic surgical staplers were then used to divide the terminal ileum intracorporeally.
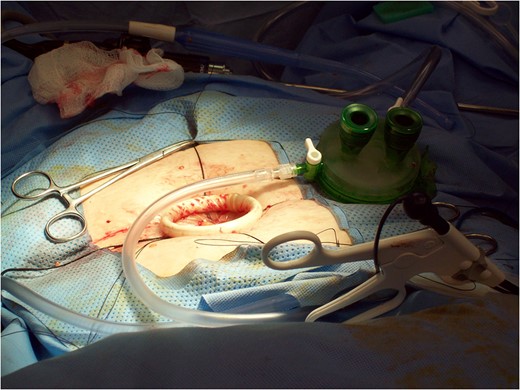
Figure 3:
Commercially available SPA.
The large bowel including the tumor was brought out through the opening in the anterior abdominal wall (Fig.
4). A side-to-side functional end-to-end ileotransverse colic anastomosis was performed with reloadable surgical staplers (Fig.
5). An enterotomy was made on the terminal ileum and a colostomy was made on the right transverse colon. Vicryl 3-0 sutures were used to bury the corners of the staple line. The anastomosis and staple line was sprayed with fibrin glue and reduced back into the abdomen.
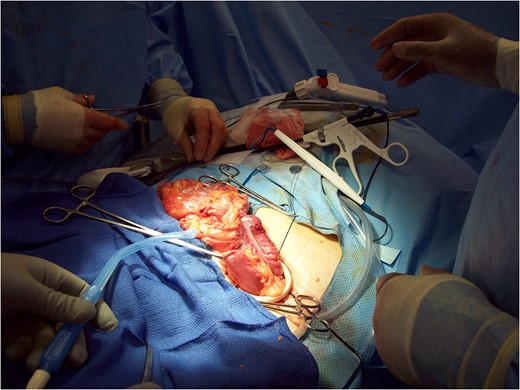
Figure 4:
Exteriorization of the ascending colon mass.
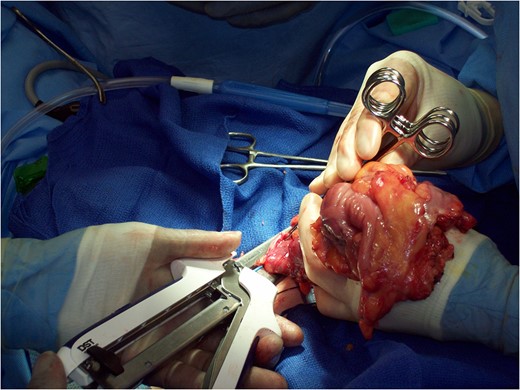
Figure 5:
Extracorporeal ileotransverse colic anastomosis.
Vaginal examination was then done to place the speculum into the vagina and put a single tooth tenaculum on the anterior lip of her cervix and an Acorn uterine manipulator at the cervix to use for manipulation of the uterus during the laparoscopic portion. Repositioning the patient for the laparoscopic approach through the SPA, the infundibulopelvic ligament, round ligament, fallopian tubes and ovaries were first divided. The broad ligaments were dissected down to the level of the uterine arteries to mobilize the structures. Hysterectomy and bilateral salpingo-oophorectomy were then completed vaginally (Figs
6 and
7). The vaginal cuff was closed by baseball stitches first then with running interlocking stitch of chromic. The cuff was closed from the superior angle to inferior angle and the uterosacral ligaments were approximated to help with vaginal vault support.
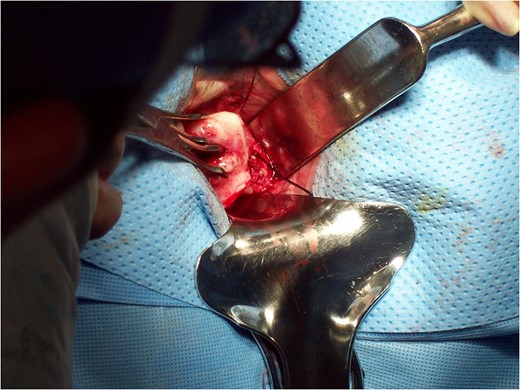
Figure 6:
Dissection of uterosacral ligament vaginally.
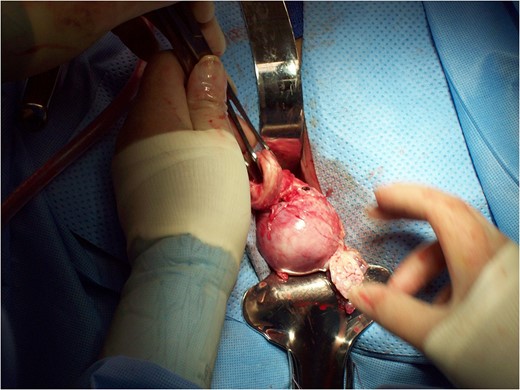
Figure 7:
Completion of vaginal hysterectomy.
The single access port was removed from the umbilicus, and the stay sutures were approximated from 9 o'clock to 3 o'clock and from 12 o'clock to 6 o'clock. Individual figure of eight sutures were placed at the fascia to avoid gaps and herniation. The skin was closed with subcuticular suture of Vicryl (Fig.
8).
Gross examination of the ascending colon showed a fungating, friable, centrally ulcerated mass 3.5 cm from the distal surgical margin that is almost circumferential and 7.5 × 4.8 × 2.1 cm in greatest dimensions. Histopathologic examination revealed infiltrating well to moderately differentiated, mucous producing adenocarcinoma, extending through the muscle wall and microscopically into the pericolonic adipose tissue with metastasis to 1/34 regional lymph nodes (Fig.
9).
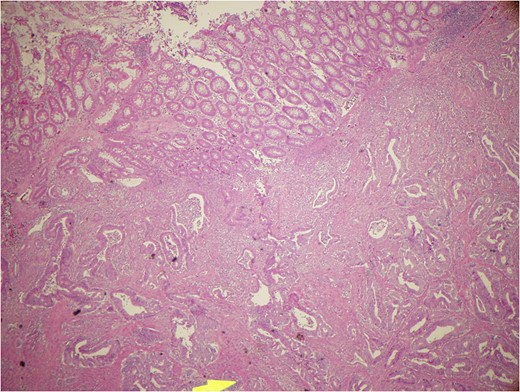
Figure 9:
Mucous producing adenocarcinoma.
Gross examination of the uterus revealed 273 g measuring 7.5 × 5.5 × 5 cm with a posterior myometrial white whorled nodule. Histopathologic examination reveals uterine leiomyoma and a benign endometrial polyp with cystic change. Final diagnosis was ascending colon adenocarcinoma Stage IIIB (T4a,N1,M0) and uterine fibroids. Postoperative course was unremarkable. Patient is currently on chemotherapy.
DISCUSSION
This is the first time, a synchronous right hemicolectomy, hysterectomy and bilateral salpingo-oophorectomy was performed through a SPA laparoscopic route. The first reported case of single incision right hemicolectomy (SIRH) was in July 2008. In 2009, Ramos-Valadez et al. recorded the first series of SIRH in consecutive unselected 13 patients with benign or malignant pathology [4]. Hirano et al. showed satisfactory lymph node harvest and resection margin and reduction in conversion rate to laparotomy with single incision laparoscopic colectomy compared with multiport conventional laparoscopic colectomy. However, there were no significant differences in short-term clinical outcomes [5].
Since the first laparoscopic hysterectomy was described in 1989 by Reich et al., initial experiences with SPA laparoscopic-assisted vaginal hysterectomy (SPA-LAVH) were documented in different countries with good postoperative outcomes [6–8]. Choi et al. [9] and Kim et al. [10] showed decreased blood loss and visual analog scale—based pain scores 24 and 36 h after surgery with SPA-LAVH compared with multiport access.
Despite the numerous advantages of SPA laparoscopic surgery, more studies are needed to determine its safety and applicability to other surgical entities especially when performing synchronous procedures.
CONCLUSION
SPA laparoscopic surgery is feasible for multidisciplinary approach in resectable tumors and achieving good postoperative outcomes.
ACKNOWLEDGEMENTS
The authors would like to acknowledge Dr K. Steven Wiley for his valuable contribution in the laparoscopic right hemicolectomy portion of the surgery.
REFERENCES
1Breitenstein
S
, Dedes
KJ
, Bramkamp
M
, Hess
T
, Decurtins
M
, Clavien
PA
.
Synchronous laparoscopic sigmoid resection and hysterectomy with transvaginal specimen removal
.
J Laparoendosc Adv Surg Tech A
2006
;
16
:
286
–
9
.
2Ramalingam
M
, King
J
, Lisa
J
.
Transvaginal specimen extraction after combined laparoscopic splenectomy and hysterectomy: introduction to NOSE (Natural Orifice Specimen Extraction) in a community hospital
.
Int J Surg Case Rep
2013
;
4
:
1138
–
41
.
3Fistarol
M
, Giostri
PG
, Noviello
MB
, Santos Filho
AS
, Wanderley Reis
MC
, Brandão
AH
.
Single incision laparoscopy using sitraccport for large adnexal mass excision and cholecystectomy: a case report
.
Med J Obstet Gynecol
2014
;
2
:
1039
.
4Valadez
R
, Gandhi
DP
, Ragupathi
M
, Patel
CB
, Ramos-Valadez
DI
, Pickron
TB
, et al. . Single Incision Laparoscopic Right Hemicolectomy: Safety and Feasibility in a Series of 13 Consecutive Cases.
Surg Endosc
2010
;
24
:
2613
–
6
.
5Hirano
Y
, Hattori
M
, Douden
K
, Ishiyama
Y
, Hashizume
Y
.
Single-incision laparoscopic surgery for colorectal cancer
.
World J Gastrointest Surg
2016
;
8
:
95
–
100
.
6Choi
YS
, Shin
KS
, Choi
J
, Park
JN
, Oh
YS
, Rhee
TE
.
Single-port access laparoscopy-assisted vaginal hysterectomy: our initial experiences with 100 cases
.
Minim Invasive Surg
2012
;
2012
:
543627
doi:10.1155/2012/543627.
7Sendag
F
, Turan
V
, Zeybek
B
, Bilgin
O
.
Transumbilical single-incision total laparoscopic hysterectomy: technique and initial experience in Turkey
.
Ginekol Pol.
2012
;
83
:
581
–
5
.
8Lee
YY
, Kim
TJ
, Kim
CJ
, Kang
H
, Choi
CH
, Lee
JW
, et al. .
Single-port access laparoscopic-assisted vaginal hysterectomy: a novel method with a wound retractor and a glove
.
J Minim Invasive Gynecol
2009
;
16
:
450
–
3
.
doi:10.1016/j.jmig.2009.03.022.
9Choi
YS
, Park
JN
, Oh
YS
, Sin
KS
, Choi
J
, Eun
DS
.
Single-port vs. conventional multi-port access laparoscopy-assisted vaginal hysterectomy: comparison of surgical outcomes and complications
.
Eur J Obstet Gynecol Reprod Biol
2013
;
169
:
366
–
9
.
doi:10.1016/j.ejogrb.2013.03.026.
10Kim
TJ
, Lee
YY
, Cha
HH
, Kim
CJ
, Choi
CH
, Lee
JW
, et al. .
Single-port-access laparoscopic-assisted vaginal hysterectomy versus conventional laparoscopic-assisted vaginal hysterectomy: a comparison of perioperative outcomes
.
Surg Endosc
2010
;
24
:
2248
–
52
.
doi:10.1007/s00464-010-0944-y.
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. © The Author 2017.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact journals.permissions@oup.com








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}