





Abstract
Meckel's diverticulum is the most common congenital abnormality of the small intestine that results from incomplete closure of the vitelline (omphalo-mesenteric) duct. This true diverticulum, ~2 ft from the ileocecal valve commonly found on the anti-mesenteric border of the ileum, is benign and majority asymptomatic. Diagnosis challenges arise when it became inflamed or presented in following ways, for example, haemorrhage (caused by ectopic pepsin—and hydrochloric acid—secreting gastric mucosa), intestinal obstruction (secondary to intussusception or volvulus) or the presence of diverticulum in the hernia sac (Littre's hernia). We report a case of a 59-year-old male who was admitted under the surgical service at Blackpool Victoria Hospital with suspected appendicitis that turned out to be a Meckel's diverticulitis, a rare presentation of an acute abdomen. We discuss the issues involved in his investigation and management as well as perform a literature review comparing different surgical approaches.
CASE REPORT
A 59-year-old man presented with a 12-h history of sudden onset of right upper quadrant and epigastric pain. The pain was then felt localized to the right iliac fossa and was constant, made worse with movement. Although he felt nauseous, he had not vomited. His last bowel movement which was 1 day previously had been normal with no bleeding per rectum noted, and no lower urinary tract symptoms.
There was no significant past surgical history. No history of recent travel and family history of colitis or inflammatory bowel disease. His medical comorbidities include Type 2 Diabetes and hypertension and his regular medications included metformin, simvastatin, ramipril, ezetimibe and lercanidipine.
On physical examination, he was pyrexial at 38.4°C, tachycardic with a pulse rate of 120 beats per minute, tachypnoeic at a respiratory rate of 20 per minute and a blood pressure of 130/70 mmHg. Clinically, he appeared flushed and in pain. His abdomen was not distended but tender and guarding in the right upper and lower quadrants. Right flank tenderness was also elicited. There were no hernias and his chest was clear.
Normal erect chest X-ray. No air under the diaphragm.
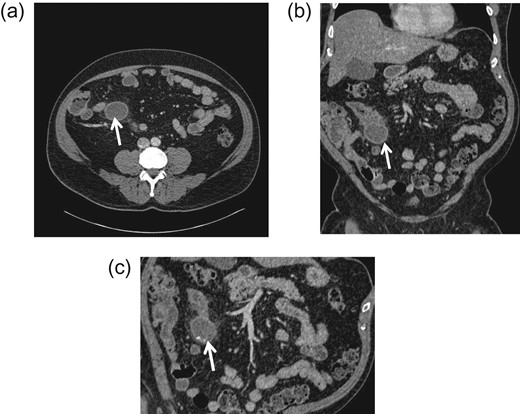
CT abdomen and pelvis (a) transverse; (b) frontal (coronal); and (c) sagittal view. An arrow indicates a blind ending sac at mid-ileal loop.
Operation

Intraoperative findings: broad based Meckel's diverticulum with oedematous adjacent small bowel (ileum).
Postoperative progress
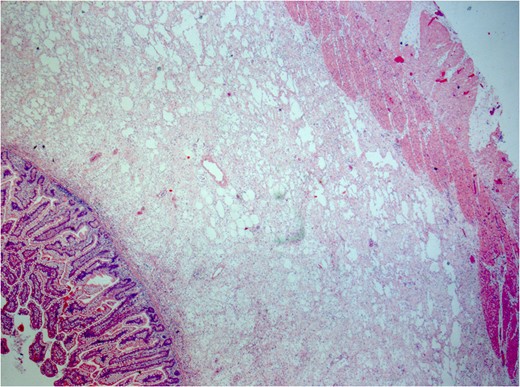
Histology: small bowel histology showing margin of resection with prominent submucosa oedema and mild inflammation.
DISCUSSION
Meckel's diverticulum is rare and accounts for only 2% of the general population. An equal incidence is found in men and women. Meckel's diverticulitis is one of the recognized complications of the condition and is clinically indistinguishable from appendicitis, except that the pain and tenderness typically localized at the periumbilical region. Progress of the diverticulitis may lead to perforation and peritonitis. A fistula between Meckel's diverticulum and the appendix has also been reported [1].
A Meckel's diverticulum is commonly discovered at operation. Resection of incidental Meckel's found during laparotomy is controversial in children and adults. It is generally recommended that asymptomatic Meckel's to be resected in children during laparotomy [2, 3] given an increased lifelong risk for complications [4]. However, this approach remains debatable in adult patients. The argument was that the likelihood of Meckel's diverticulum becoming symptomatic in an adult is 2% or less and that postoperative morbidity secondary to intestinal obstruction and infection from prophylactic resection confers no potential benefit in prevention of disease [5]. Many surgeons advocate that incidentally found normal-appearing Meckel's diverticulum should not be resected unless if there is a palpable abnormality (suggestive of the presence of ectopic mucosa), a long diverticulum (>4 cm) and a narrow neck or base of diverticulum (<2 cm wide). Elective prophylactic resection of asymptomatic Meckel's diverticulum identified on imaging is not recommended for both children and adult.
On the other hand, treatment for a symptomatic (bleeding, inflamed) Meckel's diverticulum should be prompt and referred for surgical intervention in all patients (children and adults) to relieve symptoms. The standard surgical approach is to perform a segmental (wedge or v-shaped diverticulectomy) resection of the narrow-based diverticulum or to perform a limited small bowel resection followed by primary end-to-end anastomosis if an inflamed or ulcerated diverticulum is encountered. Although gastrointestinal bleeding from a Meckel's diverticulum is a rare complication, when encountered, a segmental small bowel resection followed by end-to-end ileoileostomy rather than simple diverticulectomy is preferred [6]. Proton-pump inhibitor therapy should also be initiated on these patients. Transverse closure of the ileum with hand-sewn technique or using linear stapler across the base of the diverticulum is the ideal method to minimize the risk of subsequent stenosis.
The long-term outcomes with laparoscopy approaches (including laparoscopic diverticulectomy and laparoscopic-assisted transumbilical Meckel's diverticulectomy) are still lacking [6]. However, many studies have reported that the laparoscopic management of the complicated Meckel's diverticulum is safe, cost effective and efficient, fewer complications and shorter recovery period compared with conventional laparotomy [7, 8].
The learning point of this clinical vignette is that Meckel's diverticulitis is often clinically indistinguishable from appendicitis especially in adult patients. Computed tomography (CT) has become an invaluable tool for the evaluation of abdominal pain. CT scanning is useful in demonstrating acutely inflamed diverticula, typically identified as a blind pouch off the distal small intestine and associated with bowel wall thickening and in detecting the presence of enterocolic and enterovesical fistulas.
CONCLUSION
Open or laparoscopic diverticulectomy in managing complicated Meckel's diverticulum is safe although the latter approach depends on local technical expertise and facilities. Conservative management of an incidental Meckel's is a reasonable surgical approach.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}