





Abstract
Primary mediastinal liposarcomas are extremely rare conditions often resected through standard median sternotomy or lateral thoracotomy. However, the management of a very huge mediastinal tumor involving hemithorax through these two common surgical approaches is always challenging. Herein, we report a case of applying median sternotomy with a sternum transection plus a right fourth intercostal thoracotomy (‘⊣ shape’ incision) to resect a giant primary anterior mediastinal liposarcoma extending into the whole right thorax. The final pathological diagnosis was a well-differentiated liposarcoma. The patient experienced an uneventful recovery. The ‘⊣ shape’ incision is a good backup for the extension of standard median sternotomy and provides a better exposure for both mediastinum and hemithorax.
INTRODUCTION
Primary mediastinal liposarcomas are extremely rare, constituting <1% of all mediastinal neoplasms. These tumors grow insidiously which tend to be giant asymptomatically and extend into the pleural spaces or compress the adjacent structures, including superior vena cava and pericardium. A complete surgical resection is considered to be the optimal treatment for primary mediastinal liposarcomas [1]. A standard median sternotomy or lateral thoracotomy is the most common surgical approach. However, the management of a very huge mediastinal tumor involving hemithorax through these two common surgical approaches is always challenging. Herein, we report a case of applying median sternotomy with a sternum transection plus a right fourth intercostal thoracotomy to resect a giant primary anterior mediastinal liposarcoma extending into the whole thoracic cavity of right side.
CASE REPORT
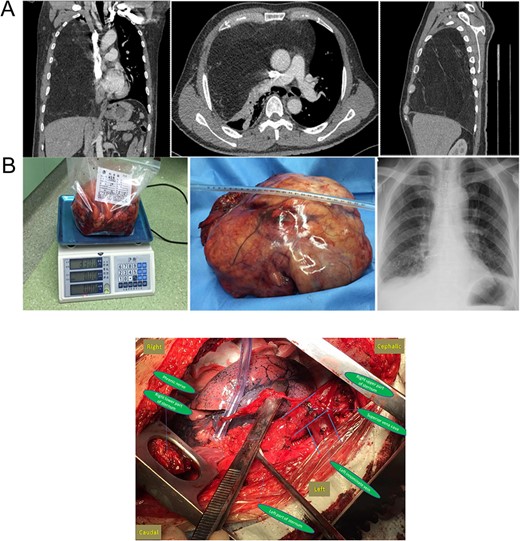
(A) Preoperative chest CT and (B) gross specimen and postoperative chest X-ray. Central Picture: “⊣ shape” incision and intraoperative surgical field after removing the giant mass.
Surgical exploration was performed first through a standard median sternotomy under general anesthesia. Dissection started from left phrenic nerve along the left innominate vein to superior vena cava. However, the giant tumor adhered severely to pericardium and the lower part of superior vena cava. Sternum transection plus a right fourth intercostal thoracotomy (‘⊣ shape incision’) was then added to guarantee a better exposure. Intraoperatively, a giant, well-capsulated yellow tumor without abundant blood supply was found, which also occupied the whole right thorax without invading the lung, chest wall, diaphragm and inferior vena cava. The main part of the tumor was smoothly removed from the right thorax after cutting off the mass along the pericardium, superior vena cava and pulmonary hilum. After careful dissection of adhesion, the rest of the tumor was gradually separated and successfully removed with partial pericardium (Central Picture). The atelectatic right lung obtained good reexpansion when both lungs were ventilated.
The gross size of the tumor was 27 cm × 20 cm × 15 cm, weigh ~3.3 kg. And it was covered with a capsule (Fig. 1B). The cut surface appeared lobulated in shape and was pale yellow in color. The final pathological diagnosis was a well-differentiated liposarcoma. The patient experienced an uneventful recovery. Postoperative chest radiography showed a normal right lung (Fig. 1B).
DISCUSSION
Liposarcoma accounts for ~9% of all primary mediastinal sarcomas with scarce data in the literature to date. Liposarcoma of the anterior mediastinum is even rarer as it is more commonly found in the posterior mediastinum [2]. Based on the limited published data, the prognosis is dependent on the histological subtype and the completion of surgical resection, with well-differentiated subtype patients exhibiting a better prognosis compared with myxoid or pleomorphic tumors [3].
Primary liposarcoma of the mediastinum remains asymptomatic until it reaches a huge size. It tends to involve the important mediastinal structures including esophagus, vessels, pericardium, etc. A standard median sternotomy or posterolateral thoracotomy is the most common surgical approaches [2, 4, 5]. In order to obtain a complete removal of the tumor, adjacent organs, such as the superior vena cava and phrenic nerve, must be mobilized.
In this case, the giant mass was located in the anterior mediastinum with much extension into the whole right thorax. For this condition, there are usually three options of surgical approaches: standard median sternotomy, lateral thoracotomy and hemiclamshell incision. Initially standard median sternotomy was performed for exploration instead of lateral thoracotomy and hemiclamshell incisions based on the following reasons: (i) the tumor was more likely to arise from anterior mediastinum; (ii) the management of large vessels in the anterior mediastinum is more challenging; (iii) exposure by those often reported hemiclamshell incisions is not satisfactory in this condition and (iv) it is easier to convert ‘⊣ shape’ incision. The giant tumor was then found to adhere severely to pericardium and the lower part of superior vena cava. It is impossible to explore the pulmonary hilar structures and right thorax. The ‘⊣ shape’ incision was then added and a better exposure was guaranteed indeed. However, if these challenges are already detected prior to surgery, a clamshell incision, semi or full, may be the much less traumatic approach for the patient.
In conclusion, to the best of our knowledge, we believe that this report is valuable because the case used ‘⊣ shape’ incision to treat such a giant liposarcoma successfully. And of course, ‘⊢ shape’ incision could be chosen for those giant liposarcomas involving left thorax. This kind of incision is a good backup for the extension of standard median sternotomy and provides a better exposure for both mediastinum and hemithorax.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}