





Abstract
We report the case of a 40-year-old woman with pseudoachondroplasia (PSACH), with a heterozygous mutation (c.806A > G, p.Asp269Gly) located in the Type 3 repeats domain of the cartilage oligomeric matrix protein gene, who complained of the unusual symptom of painful locking of the wrist. Her condition was caused by a non-traumatic enlargement of the extensor carpi radialis longus (ECRL) and brevis (ECRB) tendons along with bulbous swelling of the synoviums around them. Surgical treatment resolved these unusual tendon-related symptoms. Repetitive mechanical loading of the wrist in daily activities, including distal intersection tenosynovitis between the extensor pollicis longus tendon and ECRL and ECRB tendons, may have contributed to changes in the structural integrity of the tendons. We should pay more attention to tendon-related symptoms in patients with PSACH.
INTRODUCTION
Pseudoachondroplasia (PSACH; MIM#177170) is an autosomal dominant osteochondrodysplasia characterized by moderate to severe disproportionate short stature, ligamentous laxity and early onset degenerative joint disease. The disorder is considered to result from mutations in the gene encoding the cartilage oligomeric matrix protein (COMP; MIM# 600310) [1]. In total, 179 missense mutations have been identified in 73 of the 261 codons (28%) that comprise the T3 domain to date [2]. We report the case of a patient with PSACH with a heterozygous COMP mutation, who complained of the unusual symptom of the wrist.
CASE REPORT
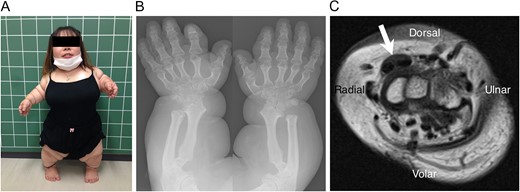
(A) The patient has disproportionate short limbs and stature (height 97 cm, weight 39 kg). (B) Plain postero-anterior radiograph of the bilateral forearms and hands. The forearm bones and phalanges are shortened, the metaphyses are widened and the epiphyses are irregularly shaped. (C) MRI of the cross-section at the level of the distal carpal row level (T1WI) shows hypertrophy of the ECRL and ECRB tendons (arrow). The synoviums around these tendons are also thickened.
Tenderness was noted over the second compartment of the dorsal wrist. Active extension of the right wrist was limited to 30° before locking occurred. Locking release was accompanied by severe pain when the wrist was passively pulled and flexed. Radiographs showed shortening of the forearm bones and phalanges, widened metaphyses and irregular and small epiphyses (Fig. 1B).
Magnetic resonance imaging (MRI) revealed hypertrophy of the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB) tendons in the second compartment. The synoviums surrounding these tendons were also thickened (Fig. 1C). We suspected that the snapping and locking of the wrist were due to impingement of the extensor tendons in this region. Based on the woman's disproportionately short limbs and stature (Fig. 1A), and other clinical characteristics, she was clinically diagnosed as having PSACH.
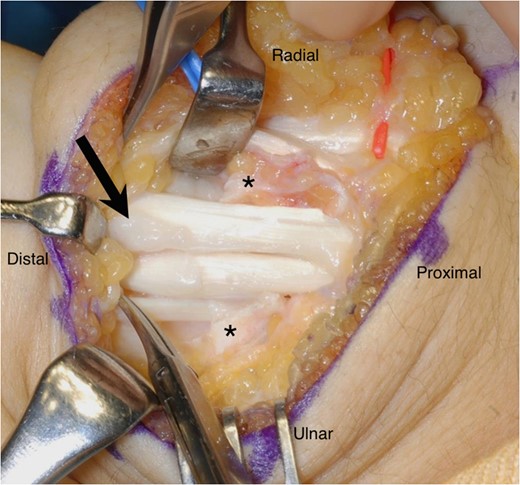
The synoviums around the ECRL and ECRB tendons appear enlarged during the surgery (arrow). Asterisks indicate the stumps of the divided extensor retinaculum.
Seven years prior to this episode, the patient had complained of identical symptoms in the contralateral wrist. She had also undergone surgery to remove the thickened synoviums around the ECRL and ECRB tendons, which had resolved the symptoms completely.
A COMP mutation in a patient with PSACH. DNA sequencing analysis demonstrates a heterozygous mutation (c.806A > G, p.Asp269Gly) in the COMP gene.
DISCUSSION
This is the first account of tendon-related symptoms reported by a patient with PSACH carrying the c.806A > G, p.Asp269Gly COMP mutation. Most of the current literature on PSACH focuses on treatment for osteoarthritis of the large joints. On the other hand, tendon-related symptoms, which originate from tendinopathy, are perhaps under recognized, since we have never encountered the literature reporting PSACH patients, in which tendinopathy is specifically mentioned. However, since COMP primarily exists in the load-bearing soft tissues, such as ligaments, tendons and skeletal muscle [3], the integrity of such structures could be attenuated in patients with PSACH.
The reasons why our patient developed unusual synovial enlargement around the tendons may be 2-fold. First, an inherent abnormality of the tendons or synovial tissues related to the COMP mutation may have been responsible. A recent animal study indicated that tendons in mutant mice were more lax as seen on biomechanical testing due to alterations in fibrillar organization and tendon cross-sectional diameter [4]. Furthermore, the pathomechanics of wrist locking in our patient were unique in that such locking in the second dorsal compartment has exclusively been preceded by apparent injury of the extensor tendons in previous reports [5, 6], suggesting that the tendons in our patient were prone to degeneration. However, we still remain unsure if this patient developed locking of the wrist due to tendon and synovial abnormalities as a phenotype of PSACH with this mutation of the COMP gene, since we did not perform any mechanical testing or examine collagen morphologies or the extracellular matrix of the affected tendon, which could have demonstrated some characteristic findings similar to the tendons in a mouse model of PSACH harboring a COMP mutation [4].
Second, repetitive mechanical loading of the wrist in daily activities, such as transferring to and from a bed and wheel chair, may have also contributed to changes in the structural integrity of the ECRL and ECRB tendons. Furthermore, it has been known that the pulley effect exerted not only by Lister's tubercle over the extensor pollicis longus tendon as it departs from the third extensor compartment and crosses over the ECRL and ECRB tendons, but also by the constraining effect of the extensor retinaculum, could affect the development of distal intersection tenosynovitis [7]. Such effects could also be responsible for tendinopathy in this patient. The possibility that the unusual configuration of the distal radius exaggerated tendinopathy could not be ruled out.
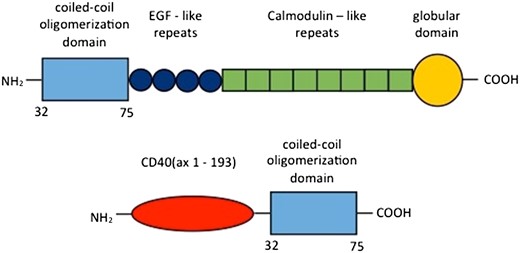
COMP is a modular protein composed of an amino-terminal coiled-coil oligomerization domain, four Type 2 epidermal growth factor-like domains, eight Type 3 calmodulin-like repeats (TSP Type-3) and a carboxyl terminal globular domain [8, 9]. COMP is strongly conserved across mammalian species and exhibits differential expression patterns at varying stages of development, suggesting that its expression is tightly controlled during transcriptional regulation and that it is an important regulator in mammalian soft tissue development [10]. The mutation identified in this patient is located in the thrombospondin (TSP) Type-3 domain, which is relatively common among COMP mutations [2]. In our comparison of protein sequences across species, COMP 269Gly was found to be highly conserved among humans, mice and rats (data not shown).
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no conflict of interest in this study.

{kind=link}
{kind=link}
{kind=link}