





Abstract
Osteomas are the most common benign osteoclastic tumours of the paranasal sinuses. However, nasal cavity and turbinate osteomas are extremely rare. Only nine middle turbinate, three inferior turbinate and one inferior turbinate osteoma cases have been reported to date. The present case report describes the management and follow-up of symptomatic bilateral inferior turbinate osteoma.
A 60-year-old female presented with symptoms of bilateral nasal obstruction and right-sided epiphora. Radiological investigation found hypertrophic bony changes involving both inferior turbinates. The patient was managed successfully by endoscopic inferior turbinectomies in order to achieve a patent airway, with no further recurrence of tumour after 3 months postoperatively.
To the best of our knowledge, this is the first reported case of bilateral inferior turbinate osteoma. We describe a safe and minimally invasive method of tumour resection, which has a better cosmetic outcome compared with other approaches.
Introduction
Osteomas are benign tumours consisting of cancellous or compact bone, with the majority of cases occurring in the skull, most commonly in the paranasal sinuses [1]. They have a predilection for the frontal (52%) and ethmoidal sinuses (22%) [2]. However, osteomas arising from the nasal turbinates are extremely rare with only 13 cases reported in the literature. We report the world's first case of bilateral inferior turbinate osteoma associated with complete nasal obstruction and epiphora in a 60-year-old female managed successfully by endoscopic bilateral turbinectomy.
Case Report
A 60-year-old lady was referred to the ear, nose and throat department with a 3-year history of complete bilateral nasal obstruction and 6 months of right-sided epiphora. Additionally, she had a pre-existing septal perforation secondary to nasal cautery for epistaxis >30 years ago. She had no significant medical history and was a non-smoker. On examination, she had massively enlarged inferior turbinates bilaterally, completely obstructing the nasal cavity. In addition, there was a 2 cm perforation of the anterior septum.
A biopsy of the inferior turbinate undertaken elsewhere reportedly showed benign cartilage and reactive looking bone. Computerized tomography (CT) of paranasal sinuses described hypertrophic bony change confined to the inferior and middle turbinates bilaterally and a deviated septum to the left. The radiological features were suggestive of a benign enchondroma involving both inferior turbinates (Fig. 1). The patient underwent endoscopic inferior turbinectomies in order to achieve a patent nasal airway. A combination of curetting and fracturing of the abnormal bone was required to achieve this. Throughout the dissection, bony adhesions were noted to the septum that needed to be divided to aid in removing the inferior turbinate. An absorbable dressing was placed with the patient instructed to perform regular saline nasal douching during the postoperative period.
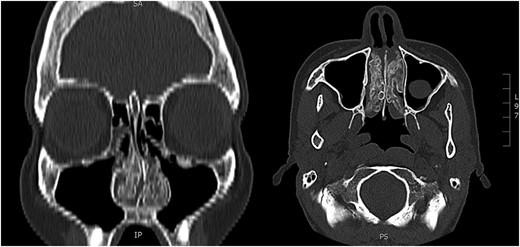
Preoperative CT. Paranasal sinuses (coronal and axial) showing bilateral inferior turbinate tumour.
Both specimens showed identical histopathological features, being composed of chronically inflamed nasal mucosa undermined and compressed by sharply demarcated, zonated, multilobulated osseous proliferation without any cartilaginous component. The core and bulk of the lesions was composed of anastomosing, cancellous type bony trabeculae separated by fibrofatty marrow spaces, surfaced by denser cortical type bone, features characteristic of benign osteoma (Figs 2 and 3).
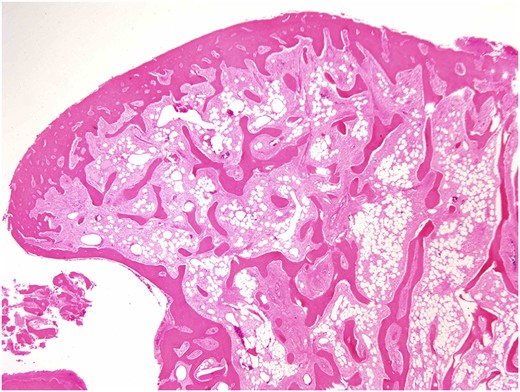
Osteoma, high-magnification photomicrograph. Scanning power photomicrograph showing disrupted pieces of multilobulated variably hyperostotic bone characterized by central anastomosing cancellous trabeculae and fibro-adipocytic interstices, surmounted by more sclerotic cortical type bone. Note the complete absence of any chondroid element (H&E stain, original magnification ×1).
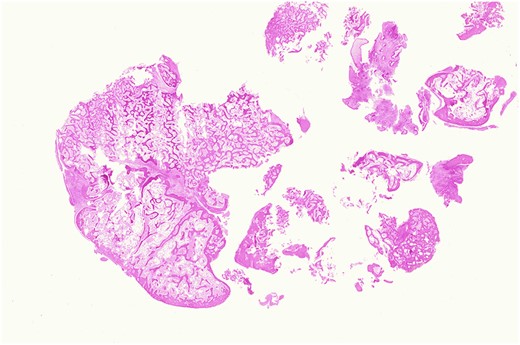
Osteoma, low-magnification photomicrograph. Low-magnification image of a protuberant bosselation emphasizing the bony zonation and total lack of haematopoietic marrow. There is neither significant osteoblastic activity nor appreciable osteoclasis (H&E stain, original magnification ×1.25).
At 3 months, she had a patent nasal airway, with resolution of nasal obstructive symptoms. Follow-up CT (Fig. 4) confirmed nasal patency and also showed non-aggressive expansion of the right middle turbinate and perpendicular plate of ethmoid, again in keeping with osteoma.
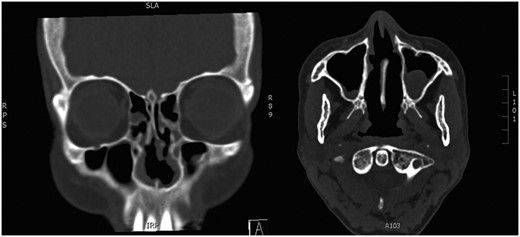
Postoperative CT. Paranasal sinuses showing patent nasal airway following bilateral inferior turbinectomies.
Discussion
Osteomas are common benign osteoblastic tumours of the paranasal sinuses that are slow growing and non-aggressive [3]. However, osteomas within the nasal cavity are very rare. To date, there are nine reports of osteoma in the middle turbinate, three of the inferior turbinate and one of the superior. We report the first ever case of bilateral inferior turbinate osteoma. All reported cases of turbinate osteoma are summarized in Table 1.
Literature review: turbinate osteomas
| Author | Date | Age | Sex | Turbinate | Approach |
|---|---|---|---|---|---|
| Daneshi et al. | 2010 | 41 | F | MT | FESS |
| Endo et al. | 2014 | 13 | M | MT | Gingival incision |
| Grabovac et al. | 2012 | 50 | M | IT | Sublabial |
| Ishimaru | 2005 | 61 | F | ST | FESS |
| Katoh et al. | 2000 | 31 | F | MT | Lateral rhinotomy |
| Kumar et al. | 2010 | 54 | F | IT | FESS |
| Kutluhan et al. | 2009 | 31 | M | MT | Craniofacial resection |
| Lin et al. | 2003 | 73 | M | MT | Lynch incision |
| Mesolella et al. | 2005 | 54 | F | IT | FESS |
| Migirov et al. | 2009 | 65 | F | MT | Refused surgery |
| Viswanatha | 2008 | 14 | F | MT | Lynch incision |
| Viswanatha | 2010 | 24 | F | IT | FESS |
| Whittet | 1988 | 31 | F | MT | Lateral rhinotomy |
| Yadav et al. | 2013 | 30 | M | MT | Lateral rhinotomy |
MT, middle turbinate; IT, inferior turbinate; ST, inferior turbinate; FESS, functional endoscopic sinus surgery.
An osteoma itself is generally asymptomatic and will not produce symptoms in its initial phase of growth, therefore is often an incidental finding or a delayed presentation. However, as it begins to increase in size within a limited and confined space such as the nasal cavity, it will produce symptoms according to mass effect. The chief complaints of nasal cavity osteoma are epiphora, epistaxis, headache and nasal obstruction. Osteoma of the middle turbinate has also been associated with pneumocephalus in one report due to tumour extension into the anterior cranial fossa [2, 4]. The differential diagnoses include enchondroma, osteochondroma, ossifying fibroma, osteoblastoma and osteosarcoma [5, 6].
The pathoaetiology of osteoma is unclear though many studies have proposed that congenital abnormalities and embryogenetic changes may play an important role [7–9]. Kaplan et al. [10] also hypothesized that muscular traction on bone may induce abnormal neoplastic change.
Three types of osteoma have been identified as compact, cancellous or mixed. They appear as radioopaque lesions on plain radiographs with a well-defined border. In the preoperative stage of management, CT of the sinuses has been shown to be the most effective imaging modality to determine the size and extent of the tumour and its relation to neighbouring structures such as the anterior cranial fossa, orbit and cribiform plate [4, 6].
Osteoma can be treated successfully by surgical excision of the tumour with no risk of recurrence [6]. Depending on the size and extent of tumour, the patient may benefit from a minimally invasive endoscopic resection of tumour such as in the present case. In eight of the cases reviewed, an open approach was considered due to the size of tumour and relationship to adjacent structures. Endoscopic surgery of the nasal turbinates carries less risk and produces a better cosmetic outcome compared to other approaches. There have been no cases of recurrence in the literature and additionally, all patients were relieved of their primary symptoms.
Nasal turbinate osteoma is an extremely rare, benign tumour. The presented case is the first ever report of a bilateral inferior turbinate osteoma. The patient underwent endoscopic sinus surgery to remove the tumour and was successfully treated. The mainstay curative treatment for osteoma is surgery and there is no risk of recurrence.
Conflicts of Interest Statement
None declared.
Funding
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}