





Abstract
Iliacus compartment syndrome is a rare retroperitoneal compartment neuropathy caused by bleeding within the iliacus muscle leading to hematoma formation and compression upon the femoral nerve, causing both sensory and motor deficits. A 75-year-old Caucasian man presented with severe right hip pain associated with motor and sensory deficit in the right lower extremity, 2 weeks post elective balloon aortic valvuloplasty for critical aortic stenosis. A non-contrast computed tomography scan revealed low-attenuation areas in keeping with an iliacus hematoma. An iliacus fasciotomy and hematoma evacuation was performed with retroperitoneal approach. The patient reported marked reduction in his groin pain with clinical improvement of the right hip flexion though the sensory deficit was unchanged. On Day 3, postoperatively the patient died from respiratory and multi-organ failure. Iliac hematomas are rare and can be caused by traumatic and non-traumatic injury, and can be exacerbated by complications of anticoagulant therapy. Delaying surgical evacuation of the hematoma can lead to prolonged or permanent disability. However, there are other reports describing good recovery with non-operative management. Non-surgical intervention is recommended if radiological studies do not explicitly confirm the presence of a discreet hematoma compressing the femoral nerve, unless progression of symptoms increases.
Introduction
Iliacus compartment syndrome (ICS) is a rare retroperitoneal compartment neuropathy caused by bleeding within the iliacus muscle leading to hematoma formation and compression upon the femoral nerve [1]. Due to the subsequent ischemia of the femoral nerve, the symptomatology of ICS follows the innervation distribution of the femoral nerve causing both sensory and motor deficits.
The pathophysiology of ICS is related to the presence of a rigid fibrous arch overlying the femoral nerve, iliacus and psoas muscles—with a potential compartment formed by four fascial planes reinforcing the distal portion of the iliacus fascia.
As a consequence of the rapid progression of the femoral nerve neuropathy, early surgical intervention by means of fasciotomy of the iliacus muscle and hematoma evacuation is the treatment of choice for clinically and radiologically confirmed ICS. We have observed three cases of ICS spontaneous on patients on anticoagulation treatment. However, we are reporting this fourth case that occurred after a femoral puncture for a coronary intervention.
Case Presentation
A 75-year-old Caucasian man was admitted for an elective balloon aortic valvuloplasty for critical aortic stenosis. He had a significant cardiac history including congestive cardiac failure, permanent pacemaker and mitral valve replacement and was on subsequent long-term warfarin anticoagulation. Interestingly, he had a prior left ICS from a spontaneous iliolumbar branch artery bleed that was treated with embolization and fasciotomy from which he made a complete recovery.
During this admission, balloon aortic valvuloplasty was attempted with right femoral artery access obtained via a right groin puncture; unfortunately, the patient became hemodynamically unstable and the procedure was abandoned. Two weeks later, the patient started complaining of severe pain in the right hip. Examination revealed extensive bruising overlying the right groin and decreased hip flexion on the right side with diminished power in the L3–S1 myotomes. Additionally, there was patchy loss of sensation to the anterior right thigh and the dorsum of the right foot. A Doppler ultrasound of the right groin was performed which revealed a 2 cm false aneurysm in the right groin medial to the right common femoral artery. A non-contrast computed tomography (CT) scan was also performed which revealed areas of mesenteric stranding in the right iliac fossa with an enlarged right iliacus muscle measuring 7 × 6.5 cm. The iliacus muscle demonstrated subtle low-attenuation areas in keeping with an iliacus hematoma (Fig. 1a and b).
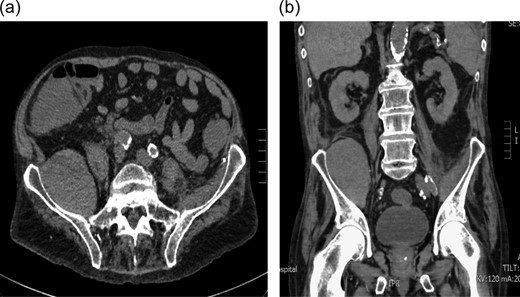
(a and b) Axial and coronal computerized tomography scans demonstrating a large iliacus hematoma in the right iliac fossa.
Ultrasound guided thrombin injection was performed to treat the pseudoaneurysm. A follow-up CT angiogram demonstrated successful thrombosis of the right CFA pseudoaneurysm and a stable iliacus hematoma with no active iliac arterial extravasation. The patient was taken to the operating theater for an iliacus fasciotomy and hematoma evacuation.
On exposure, the retroperitoneal layer was reflected medially and the neurovascular structures were identified and protected. The right iliac vessels were visualized and no active bleeding was seen. A complete fasciotomy of the iliacus compartment was performed and approximately 400 ml of hematoma was evacuated. The anterior abdominal wall was closed in two layers and two drains were inserted into the retroperitoneal space.
The patient was admitted to ICU due to respiratory acidosis. He was extubated on postoperative Day 1 and reported marked reduction in his groin pain. He also demonstrated clinical improvement in his right hip flexion though the sensory deficit was unchanged. Unfortunately, on postoperative Day 2 he began deteriorating, requiring increasing inotropic support and ventilatory support with respiratory failure. The following morning the patient passed away from multi-organ failure.
Discussion
ICS is characterized as a retroperitoneal compartment neuropathy caused by bleeding within the iliacus muscle leading to hematoma formation and compression upon the femoral nerve. It should be noted that these hematomas can be caused by traumatic and non-traumatic injury, and can be exacerbated by complications of anticoagulant therapy [1]. The incidence of this condition is rare; Tamai et al. [2] reported only 35 cases of traumatic injury in the literature between 1942 and 1999 of which 24 cases were analyzed, moreover, Dauty et al. [3] reported an incidence on 2.9 per 1000 in patients with moderate to severe hemophilia.
As the femoral nerve emerges from the pelvis in a groove deep to the iliacus fascia between the iliacus and psoas muscles, increased pressure upon this nerve can reveal significant adverse neurological affects. The hematoma providing this pressure is created within the potential compartment formed by four fascial planes creating three distinct fascial compartments (dorsal, intermediate and ventral) reinforcing the distal portion of the iliacus fascia [4].
In this case, the patient experienced both sensory and motor deficits in the regions described, and an early fasciotomy with hematoma evacuation was indicated to provide decompression of the compartment to facilitate femoral nerve recovery [5]. Delaying surgical evacuation of the hematoma can lead to prolonged or permanent disability [6]. Holscher et al. [7] described two cases whereby drainage of the hematoma was performed percutaneously using ultrasound guidance, however, this can only be performed if the hematoma remains unclotted [1]. In the paper by Weiss and Tolo [8], non-surgical intervention is recommended if radiological studies do not explicitly confirm the presence of a discreet hematoma compressing the femoral nerve, unless progression of symptoms increases. Overall, with the limited data available, of the 24 cases analyzed by Tamai et al. [2], 19 patients were treated surgically of which 14 patients (74%) achieved complete neurological recovery of the femoral nerve with the balance resulting in incomplete or variable recovery.
An interesting feature in our case was the patient's history of previous ICS on the contralateral side. Given the rarity of this condition, perhaps there are anatomical patient characteristics that are risk factors in addition to anticoagulation. ICS is a rare but significant entity as the consequences of delayed treatment can lead to prolonged or permanent disability. Good clinical acumen and prompt imaging on suspicion can facilitate early detection.
Consent
‘Written informed consent was obtained from the patient's next of kin for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.’
Competing Interests
The authors declare that they have no competing interests.
Authors’ Contributions
Our patient was admitted under the care of PT during this episode. AP was major contributor in writing the manuscript. All authors read and approved the final manuscript.

{kind=link}