





Abstract
Blunt abdominal trauma causing gallbladder rupture is exceptionally rare in children. This injury is rare due to the size and anatomical location of the gallbladder, and a rapid diagnosis is often difficult to achieve due to delayed presentation. We report a ruptured gallbladder in an 11-year-old male as a result of blunt abdominal trauma from an all-terrain vehicle accident. Possible gallbladder injury was indicated on computed tomography and patient was successfully managed with cholecystectomy.
Introduction
Blunt abdominal trauma causing gallbladder rupture is exceptionally rare in children [1]. Because the gallbladder is anatomically protected by the liver and ribs, only ~2% of patients who undergo laparotomy are found to have gallbladder injury [2, 3]. Diagnosis of injury is most commonly made during exploration of other serious concomitant injuries. With isolated injuries, the diagnosis is often delayed since the onset of symptoms may not develop acutely. Patients may not seek treatment until several days to weeks after the injury. When presentation is delayed, patients often develop severe abdominal pain, nausea, vomiting and jaundice. Gallbladder injury is most commonly confirmed by computed tomography (CT) scans, and the presence of pericholecystic fluid in these images strongly suggests injury to the gallbladder [4].
We report a ruptured gallbladder in an 11-year-old male as a result of blunt abdominal trauma from an all-terrain vehicle (ATV) accident. Possible gallbladder injury was indicated on CT and patient was successfully managed with cholecystectomy.
Case Report
An 11-year-old male was transferred from an outside hospital to our Level 1 pediatric trauma center following a non-traffic ATV accident.
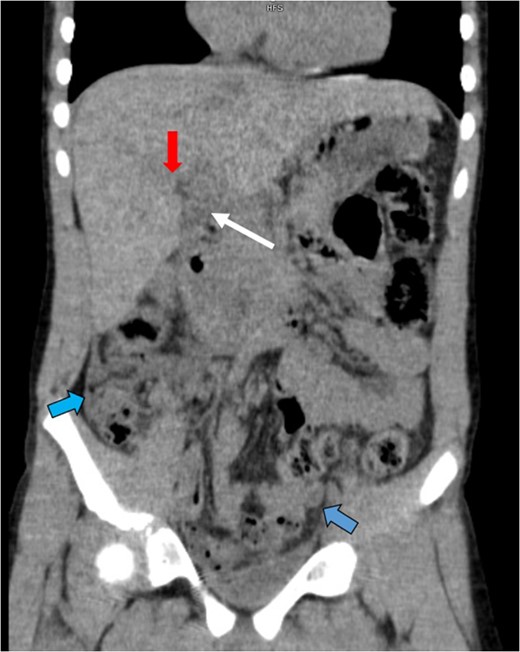
An abdominal CT showed a collapsed gallbladder with wall thickening or pericholecystic fluid (white arrow), a grade II hepatic laceration of Segment 5 (red arrow) and an increased amount of free fluid in the abdomen (blue arrows).
Discussion
Few cases of gallbladder injury due to blunt abdominal trauma have been reported in pediatric patients. This injury is rare due to the size and anatomical location of the gallbladder, and a rapid diagnosis is often difficult to achieve due to delayed presentation.
CT scans are typically the imaging modality of choice following abdominal trauma in a stable patient; however, diagnosing gallbladder injury can be challenging [5]. An anomalous contour of the gallbladder wall, collapsed lumen or presence of pericholecystic fluid on these scans strongly suggests primary injury to the gallbladder [4]. The presence of bile in the peritoneum is another potential indicator of gallbladder damage. The majority of patients with gallbladder injury will also have concomitant injuries to the liver, bowel, pancreas or other intra-abdominal organs, prompting exploratory laparotomy. Injuries affecting the duodenum and bile ducts can also lead to bile in the peritoneal fluid, so no definitive conclusions may be drawn from the finding of bile in the peritoneum. While mortality due to gallbladder injury is rare, a mortality rate as high as 24% has been reported due to injuries that occurred at the same time as gallbladder damage [6]. The prevalence of other serious injuries associated with gallbladder rupture suggests that the majority of these patients should undergo exploratory laparotomy. Evaluation of the extra-hepatic bile ducts should also be performed [7]. Cholecystectomy remains the accepted management strategy for patients with this injury.
For blunt trauma, gallbladder injuries can be classified as contusions, avulsions or most commonly lacerations, which include perforations and ruptures [8]. Our patient's injury was classified as a laceration. Healthy gallbladders can be more vulnerable to injury compared with diseased gallbladders that are chronically inflamed or fibrotic. Because damage to a healthy gallbladder will typically result in the leakage of sterile bile, symptoms may not present acutely, and the onset of symptoms may be delayed for several weeks. Individuals in a fasted state are also more susceptible to injury because the gallbladder wall is typically more distended after several hours without food.
We report a case of gallbladder rupture following blunt abdominal trauma in a pediatric patient. CT scans showing an abnormal contour of the gallbladder and presence of bile in the peritoneal fluid are strong indicators of primary gallbladder injury. Exploratory laparotomy with cholecystectomy is an effective method of surgical management for patients with this injury.
Conflict of interest statement
None declared.

{kind=link}