





Abstract
Primary dedifferentiated liposarcoma originating in the mediastinum is extremely uncommon. Here, we report a case of mediastinal dedifferentiated liposarcoma. A 74-year-old man was admitted to our hospital with a left intrathoracic tumor ∼10 cm in diameter. Computed tomography that was taken in another hospital 2 years before the initial visit to our hospital had shown a lipomatous tumor ∼3 cm in diameter adjacent to the left lower pulmonary vein. The tumor was resected by left lateral thoracotomy with video-assisted thoracoscopic surgery. Pathological examination revealed primary mediastinal dedifferentiated liposarcoma. No evidence of recurrence has been seen as of 8 months postoperatively.
INTRODUCTION
Primary liposarcoma of the mediastinum is uncommon among mediastinal malignant neoplasms. About 90–95% of liposarcomas occur in the trunk, extremities or retroperitoneum, while primary mediastinal liposarcoma is extremely rare. Mediastinal liposarcomas comprise 0.1–0.75% of all mediastinal tumors [1]. Liposarcoma has been subclassified histologically into well-differentiated type as an intermediate malignancy, and dedifferentiated, myxoid, pleomorphic and not otherwise specified, as malignant adipocytic tumors.
CASE REPORT
A 74-year-old man was referred to our hospital after a left middle and posterior mediastinal tumor was detected on computed tomography (CT) performed as an examination for dry cough in other hospital. CT about 2 years earlier had shown a 3.2 × 2.4-cm lipomatous tumor at the left hilum adjacent to the left lower pulmonary vein (Fig. 1), and that lipomatous tumor was considered the origin of the present mediastinal tumor. Contrast-enhanced CT performed in our hospital showed a heterogeneous tumor, displacing the left lower lobe of the lung, and measuring 10 × 7.4 × 6 cm on horizontal and coronal sections (Fig. 2A and B). Magnetic resonance imaging showed a hyperintense marginal region with central hypointensity on T1-weighted imaging, and heterogeneously high intensity in the whole tumor on T2-weighted imaging. We scheduled surgical resection, and the patient was admitted to our hospital 3 weeks after the first visit. Chest radiography showed rapid growth of the left intrathoracic tumor (Fig. 3A and B), and CT revealed a tumor measuring 11.4 × 8 × 6.2 cm without pleural effusion or hemothorax.

CT from another hospital 2 years earlier shows a 3.2 × 2.4-cm lipomatous tumor at the left hilum adjacent to the left lower pulmonary vein.
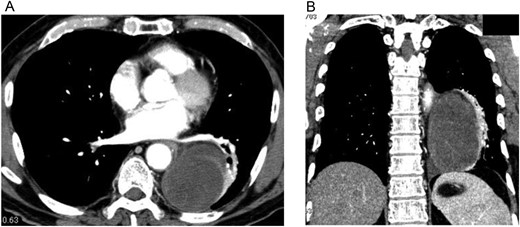
Contrast-enhanced CT of the chest shows an oval, smooth-shaped, heterogeneous tumor displacing the left lower lobe of the lung, measuring 10 × 7.4 × 6 cm on horizontal (A) and coronal (B) sections without pleural effusion or hemothorax.
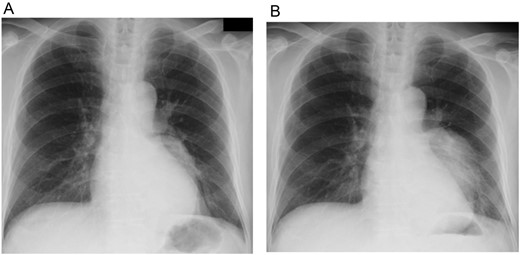
Chest X-ray from the first visit to our hospital (A), and 3 weeks after that initial visit (B). These photos show rapid growth of the left intrathoracic tumor.
Extirpation of the tumor was performed with a 15-cm left lateral incision assisted with a thoracoscope. The tumor appeared smooth and encapsulated, and appeared to have originated from mediastinal fat tissue. No adhesion between the tumor and descending aorta was evident, although fibrous adhesion between the tumor and lung was present without direct invasion. Grossly, the extirpated tumor was well circumscribed, ∼11 × 8 × 7 cm in size and encapsulated by thin, fibrous tissue. The cut surface revealed a myxoid appearance, partially intermingled with a whitish, solid part (Fig. 4). Histopathologically, the myxoid area showed proliferation of pleomorphic tumor cells such as plump spindle-shaped cells, stellate cells and large atypical cells with bizarre nuclei, embedded in myxoid stroma. The whitish, fibrous part comprised dense fibrous stroma containing scattered pleomorphic tumor cells and partially intermingled with mature fat tissue, showing features of well-differentiated liposarcoma (Fig. 5A and B). Immunohistochemistry revealed positive nuclear staining for CDK4 and MDM2 in both myxoid and fibrous parts of the tumor (Fig. 5C and D). Dedifferentiated liposarcoma was therefore diagnosed.

Gross appearance of the tumor. The well-circumscribed mass is encapsulated by fibrous tissue, showing a myxoid appearance intermingled with a whitish, solid part on the cut surface.
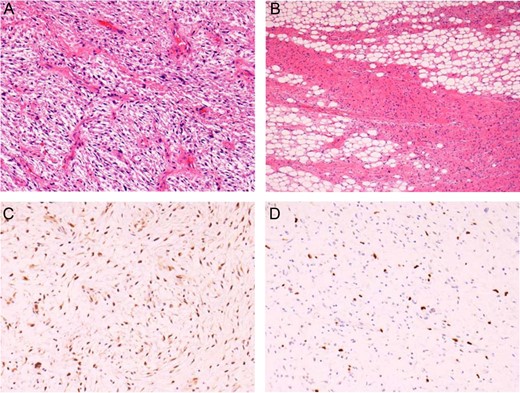
Histopathological findings of the tumor. (A) Myxoid, pleomorphic component. (B) Well-differentiated liposarcoma component. Positive immunoreactions for CDK4 (C) and MDM2 (D) in the nuclei of tumor cells, confirming the diagnosis of dedifferentiated liposarcoma.
The postoperative course was uneventful, and the patient was discharged on Postoperative Day 6. No evidence of recurrence has been identified as of 8 months postoperatively.
DISCUSSION
Sarcomas are heterogeneous neoplasms that display diverse biological behaviors, and many show unique genetics. Liposarcoma is the most common soft tissue sarcoma arising from numerous anatomic sites. About 90–95% of liposarcomas occur in the trunk, extremities or retroperitoneum, but primary mediastinal liposarcoma is extremely uncommon. Primary intrathoracic liposarcoma represents 2.7% of all sites. Furthermore, mediastinal liposarcoma comprises 0.1–0.75% of all mediastinal tumors [1] and ∼9% of primary sarcomas of the mediastinum [2–4].
Histologic heterogeneity is seen within the liposarcomas. Liposarcoma is subclassified into five histologic subtypes: dedifferentiated, myxoid, pleomorphic, and not otherwise specified as malignant adipocytic tumors; and well-differentiated liposarcoma as an intermediate malignancy according to the latest World Health Organization classification. Approximately 90% of dedifferentiated liposarcomas arise de novo and 10% develop as recurrences. Dedifferentiated liposarcoma can be identified histologically by the transition from well-differentiated liposarcoma to nonlipogenic sarcoma, and the dedifferentiated areas demonstrate variable histological characteristics [5].
The histological type of liposarcoma was considered to affect the prognosis of this neoplasm, with the dedifferentiated type regarded as a highly malignant tumor with a tendency toward local recurrence and metastasis [1]. Rekhi et al. reviewed 25 cases of dedifferentiated liposarcoma and noted that liposarcoma should be carefully examined for dedifferentiated components—which show a wide spectrum, including low- and high-grade types—considering this tumor is aggressive, irrespective of the grade of dedifferentiation. They considered dedifferentiated liposarcoma as an uncommon sarcoma with a wide histopathological spectrum and unfavorable clinical course [6].
Dedifferentiated liposarcoma is a heterogeneous tumor that can appear similar in morphology to various sarcomatous neoplasms, but is usually adjacent to a well-differentiated liposarcoma component. Nevertheless, in rare cases, the transition from well-differentiated liposarcoma to dedifferentiated liposarcoma cannot be observed histologically. Recently, immunohistological and/or molecular analyses have been used to confirm the diagnosis, to show overexpression of proteins or amplification of CDK4 and MDM2 genes on chromosome 12q [3, 7].
At present, liposarcomas, including dedifferentiated liposarcomas, are recognized to show poor response to chemotherapy and radiotherapy, so the best treatment for dedifferentiated liposarcoma appears to be complete surgical resection. Ifosfamide and doxorubicin are the most frequently used chemotherapeutic agents in patients with mediastinal liposarcoma. However, the use of adjuvant treatments for mediastinal liposarcoma remains controversial [1, 4].
Because liposarcoma responds poorly to systemic chemotherapy, novel molecular targets need to be identified to provide new therapeutic possibilities. Dedifferentiated liposarcoma and well-differentiated liposarcoma are characterized by the amplification of genes on chromosome 12q, MDM2 and CDK4, and targeting of MDM2 and CDK4 is an active area of clinical research [8].
In this report, we have described a case of mediastinal dedifferentiated liposarcoma originating from the hilum, showing rapid growth over 3 weeks preoperatively and resected by left lateral thoracotomy with video-assisted thoracoscopic surgery. Although research has focused on therapies targeting genes on chromosome 12 for the potential to manage the liposarcoma, complete surgical resection remains the most effective treatment for mediastinal dedifferentiated liposarcoma.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}