





Abstract
Cutaneous metastasis (carcinoma en cuirasse) is a condition that results from a tumor spreading via lymphatic or vascular embolization, direct implant during surgery or skin involvement by contiguity. Contralateral distant cutaneous breast cancer has never been reported before and hence, the nature and management of such rare cases remains challenging. We aim to present a case of left-sided ‘distant’ cutaneous metastatic invasive duct carcinoma affecting the distal upper extremity (contralateral side) two and half years (disease-free) following treatment for right breast cancer (right mastectomy + chemoradiation). A complete metastatic work-up excluded the presence of any underlying disease. Clinical examination revealed a fungating, irregular ulcer that bled easily on touch involving the left forearm. The ulcer was excised totally and the raw area reconstructed using a split thickness graft. The patient had uneventful postoperative course and now remains disease-free for almost 1 year with no evidence of local recurrence.
INTRODUCTION
Breast cancer involving the skin is considered an advanced disease [1]. However, rare case reports have described ipsilateral cutaneous metastasis following successful treatment of primary breast cancer [2]. The explanation of such mechanism when affecting the ipsilateral side remains either vascular or lymphatic permeation [2, 3]. Contralateral cutaneous breast cancer has barely been reported before and hence, the nature and management of such rare cases remains challenging to the breast surgeon.
CASE REPORT
A 36-year-old female presented to the surgical outpatient clinic of the National Cancer Institute (NCI—Cairo University) with a rapidly growing fungating left forearm cutaneous lesion. Her past medical history was significant for invasive ductal carcinoma of the right breast. She underwent right-sided mastectomy followed by chemotherapy and radiotherapy that dated two and half years prior to this presentation. Clinical examination revealed a fungating, irregular ulcer involving the left forearm that bled easily on touch. The ulcer measured 7 cm × 9 cm in maximum dimension, had an irregular outline and was fixed to the underlying extensor forearm muscles. Examination on the left breast including the axilla revealed no suspicious masses or cutaneous lesions. Incisional biopsy of the ulcer showed the presence of metastatic duct carcinoma. Complete metastatic work-up including left breast imaging (digital mammography and ultrasound) and computerized tomography of the chest, abdomen and pelvis excluded the presence of any underlying disease. The case was discussed in our breast multidisciplinary team (MDT) meeting and plan for resection was formulated.
The patient had surgery to excise the left forearm ulcer. The raw area left following excision was covered using a split thickness graft. Postoperative gross and microscopic pathology confirmed our primary diagnosis (distant metastatic cutaneous invasive duct carcinoma). The patient had an uneventful postoperative course and was discharged on the third postoperative day. She now remains disease-free for almost 1 year with no evidence of local recurrence (Figs 1–5).

Preoperative.
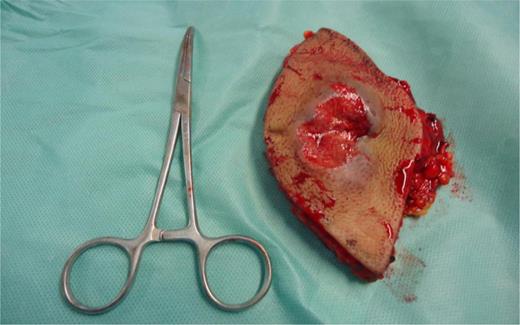
Surgical specimen.
![Surgical bed [forearm] after excision.](https://oupdevcdn.silverchair-staging.com/oup/backfile/Content_public/Journal/jscr/2015/6/10.1093_jscr_rjv062/2/m_rjv06203.jpeg?Expires=1785925439&Signature=MBLTHZSvnqzySuHNldKy6girD5ulHrCECdyFHln8xWit6iFYyJgvePemGpl5F1fOdxyBJuWyeUNH10vmQToIJHKsMt0-kKec6CPWHru6sydBAqd6yq3HeEaVQsaFdaVb5CjSz1CUGxzIIM7DZpy1aq4C2w1cOljDrkn3PipvbJebsv8L18Gni9mq21D4gGNyXjN7QVkjy~7gg~y0PdoSIlGOFp2jw0ZdiZaPlfjqItpdcrbJbwSpaeLYVTZ~A7xe0IJioHs~GZvLipgsu266m67co9028YXNzTPsNmcdLwAzxQU3-w0MCyVdW-UT8IuzDf67dQBiJEbaFtBS~Amufw__&Key-Pair-Id=APKAIYYTVHKX7JZB5EAA)
Surgical bed [forearm] after excision.

Immediate postoperative.

Six months postoperative.
DISCUSSION
The skin is an uncommon site for distant metastasis, with breast, lung and colon representing the most common primary site of cancer. Such lesions when discovered usually indicate disseminated disease and carry a poor prognosis [4]. Carcinoma en cuirasse is a rare described form of metastatic cutaneous carcinoma (0.6–10%) that results from a tumor spreading via lymphatic or vascular embolization, direct implant during surgery or skin involvement by contiguity. Cutaneous metastasis in breast cancer is most commonly linked with local recurrence post mastectomy; however, it may rarely appear as the presenting feature of breast carcinoma [1].
During the early weeks of embryonic development, the mammary milk lines extend from the axillary region to the groin. In normal development, most of the mammary ridges resolve except for two segments in the pectoral region, which later on become the breasts [5]. Failure of any portion of the mammary ridge to involute will result in the existence of ectopic breast tissue [5]. The possibility of a second primary ectopic breast cancer may be entertained in patients with prior history of breast cancer when a new malignant lesion is found in the milk line distribution. However, very rarely extra-mammary nipples have been reported in locations outside the milk line [6]. Thus, the remote possibility of the extremity lesion noted in our patient being a primary ectopic cannot be excluded.
None of the large scale studies from the past three decades that have described cutaneous metastasis have mentioned involvement of contralateral distant sites with metastatic breast cancer in the absence of local ipsilateral disease [7, 8]. The diagnosis and management of such cases remains challenging owing to its rarity. The value of neoadjuvant chemotherapy prior to surgery is debatable. The lack of local recurrence or active metastatic disease elsewhere and the rapid course of the fungating cutaneous deposit encouraged the MDT committee to opt for a surgical excision prior to chemotherapy.
It is difficult to explain why such a cutaneous deposit has evolved distantly to the primary cancer site; yet, we can only speculate the presence of extensive network of breast lymphatics that might have cross-communicated over the course of time.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}