





Abstract
We present the case of a 23-year-old man who consulted in the emergency department 6 days after ingesting a wooden toothpick with features of a localized peritonitis in the left upper quadrant of the abdomen. Surgical exploration revealed a perforation of the splenic flexure of the colon by the toothpick during its migration. This rare case is analysed in the light of the current literature. There is need for a greater awareness about the dangers of a swallowed toothpick. It is advisable to always trace the toothpick until it is found or expelled.
INTRODUCTION
Foreign bodies accidentally or intentionally ingested usually pass the entire gut without incidents. Sharp objects such as a toothpick sometimes fail to pass and may cause a perforation. This type of unusual injury may cause significant morbidity and mortality. The possible complications reported in the literature include obstruction, perforation, haemorrhage, fistula formation and sepsis [1].
Toothpick injury to the gut is a rare condition for which a low intellectual quotient and extremes of age have been described as predisposing factors [2]. The most common mode of presentation is abdominal pain [2]. Diagnosis is made difficult by the fact that few patients remember swallowing a toothpick, the delay before onset of symptoms is extremely variable [3], the physical and laboratory findings are unspecific and the injury is frequently caused by a wooden toothpick which is radiolucent [1]. The most frequently reported locations for toothpick-related perforation of the gut include the caecum, sigmoid colon, duodenum and stomach. Other locations are rarer. The management still require a laparotomy in a majority of cases [3].
We present the case of a patient who sustained a perforation of the splenic flexure of the colon by a wooden toothpick accidentally ingested.
CASE REPORT
A 23-year-old otherwise healthy student is brought by his mother to the emergency department for a left-sided burning abdominal sensation 6 days after accidentally ingesting a wooden toothpick. He initially consulted in a health centre immediately after the incident with no symptoms and was advised to go back home. His mother insists on telling us that she thinks the toothpick is the cause of the problem.
Physical examination reveals normal vital signs and tenderness on deep palpation of the left flank. No lump is palpated. Plain abdominal X-ray is normal. Full blood count elicits a leucocytosis (11 400/mm3, 86% of neutrophils), and abdominal ultrasound reveals an agglutination of bowel around the splenic flexure of the colon, but no foreign body is identified.
A mini-laparotomy performed 18 h after admission shows localized peritonitis in the left hypochondrium with the greater omentum and a small bowel contributing to circumscribe the infectious process. A wooden toothpick is discovered, partially in the peritoneal cavity, perforating the anti-mesenteric border of the splenic flexure of the colon (Fig. 1 ). The toothpick is removed (Fig. 2) and the perforation of the colon closed with an absorbable polyglactin suture and protected with an omentum patch.
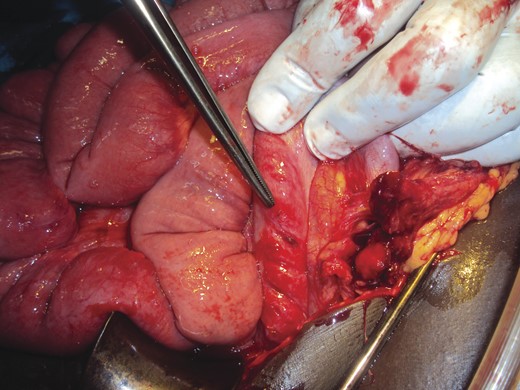
A peroperative view showing the colonic perforation (tip of the forceps).

The wooden toothpick immediately after removal.
The postoperative period is uneventful and the patient is discharged home after 7 days.
DISCUSSION
Ingested toothpicks very rarely cause perforation of the gut. The incidence of this type of lesion has been reported to be 0.2 per 100 000 people every year in the USA [4].
Our patient displayed none of the previously described related factors such as dementia, young or old age or carriage of denture [2]. It is likely that this young man continued to play with the toothpick after use.
Longer delays between ingestion of the toothpick and diagnosis have been described previously [2, 3]. According to Li and Ender [3], the delay ranges between 1 day and 15 years!
Swallowed toothpicks are likely to cause a variety of lesions including perforation, bleeding, obstruction and haemorrhage [2, 3]. Septic complications have also been described [1], sometimes related to the migration of the toothpick out of the digestive tract [3].
All the portions of the gut could be concerned by the perforation [1, 5–8], but they more frequently occur in areas controlled by sphincters, physiological narrowing and acute flexures [2]. The most commonly described locations include the caecum [6], the duodenum, the sigmoid and the stomach [3, 6–8]. The occurrence in the splenic flexure of the colon is very rare [3].
The diagnosis is not always obvious; it has been reported that the toothpick could be unnoticed in >80% of cases [3]. In our case, the mother kept repeating: ‘it is the toothpick!’
Most patients consult for an abdominal pain, usually non-specific [3] and often misleading [2, 3]. Standard X-ray studies usually fail in identifying the toothpick. As in our patient, many cases are diagnosed or confirmed only during laparotomy or endoscopy [2, 3, 7, 8].
Once this condition is diagnosed, the treatment is usually easy and the recovery uneventful [2, 7, 8]. Endoscopic treatment should be preferred to surgery whenever possible [2].
A mortality rate as high as 18% has been reported [3].
This case indicates that there is need to increase awareness of healthcare providers and populations on the potential dangers of an ingested toothpick. Each time this incident occur, it is advisable to follow-up such patients until the foreign body is properly traced as it may cause damage even months or years after. They could account for significant morbidity and mortality.
CONFLICT OF INTEREST STATEMENT
A.C.-M. has no conflict of interest to disclose.

{kind=link}
{kind=link}