





Abstract
Lipomas are found most often on the torso, neck, upper thighs, upper arms and armpits; they can also occur almost anywhere in the body. Parietal peritoneum lipoma is a rare intraoperative finding during abdominal surgery. We present a case of a torted, pedunculated parietal wall lipoma in the right iliac fossa that gave rise to a clinical diagnosis of appendicitis. So far only one case has been reported.
INTRODUCTION
Lipoma is benign mesenchymal tumor of soft tissue that composes mature fat cells. Solitary lipomas are seen predominantly in women, whereas lipomatosis occur more frequently in men. It can occur throughout the whole body [1, 2]. Most lipoma becomes apparent between the ages 40 and 60 years. The superficially frequently affected regions are the neck, back and proximal extremities [3]. Deep lipoma can affect thorax, mediastinum, chest wall, pelvis, retroperitonium and paratesticular regions [4].
In the gastrointestinal tract, lipomas are found in submucosa and subserosa and act as a leading point for intussusceptions. Intraperitoneal lipoma is rare and few have been reported as parietal peritoneal lipoma.
CASE REPORT
A 32-year-old male came to emergency department following pain in the right iliac fossa (RIF) for 1 day. The pain was intermittent and non-radiating. There was a significant decrease in appetite, but no nausea and vomiting. He had no fever, upper respiratory tract symptoms or urinary symptoms.
On examination he was noted to have guarding and localized rebound tenderness in RIF. The rest of his examination was unremarkable. Routine pathology showed white cell count of 10.2 × 107/l. Ultrasonography (USG) of abdomen showed mild deep probe tenderness in RIF.
He was admitted with provisional diagnosis of appendicitis and commenced on intravenous fluid and antibiotic overnight. Next morning he complained of pain being constant and signs of peritonism were present for which he was prepared for theatre. He proceeded to laparoscopic appendectomy that morning. Upon laparoscopy the appendix was not grossly inflamed (Fig. 1). But a torted pedunculated lipoma of 3 cm size was noted on right lower quadrant parietal peritoneum (Fig. 2). Laparoscopic appendectomy with excision of torted lipoma was done. The patient was discharged on the third postoperative day after an uneventful recovery. His histopathology report showed lymphoid hyperplasia of appendix. Peritoneal lesion smear showed mature adipose tissue in lobules separated by fibrocollagenous tissue and few congested blood vessels.
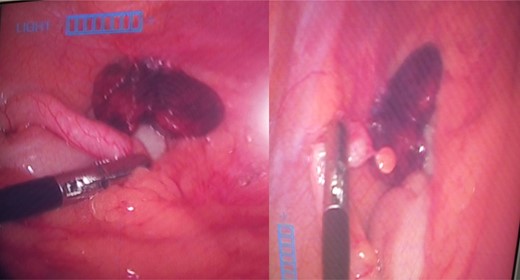
Intraoperative images showing normal appearing appendix with torted parietal peritoneal lipoma.

Intraoperative image showing torted ischemic parietal peritoneum lipoma in RIF.
DISCUSSION
Acute abdominal pain is the most common case of hospital admission accounting for 5 to 10% of all emergency department visits [5]. Acute abdomen generally refer to previously undiagnosed pain that arises suddenly and is of <48 h duration that seeks medical attention [6].
Acute appendicitis is the most common abdominal surgical emergency performed annually. Various other diseases can give rise to features suggesting acute appendicitis. As in this case, a torted lipoma of parietal peritoneum mimicked as acute appendicitis.
Lipoma is the most common benign form of soft tissue tumor composed of adipose tissue. Lipomas are generally soft to touch, usually movable and painless. Approximately 1% of the general population has a lipoma. One percent of lipoma has a tendency for malignant transformation and is more likely in lesions of lower extremities, shoulders and retroperitoneal areas.
More than half of lipomas encountered by clinician are subcutaneous in location. Commonest subcutaneous lipomas are not a serious condition. Lipomas of an internal organ can be dangerous as in the gastrointestinal tract, leading to bleeding, ulceration and obstruction. Others like lipoma of the superior vena cava, brain and spinal cord can pose a significant clinical challenge.
Primary peritoneal tumors are uncommon lesions that arise from mesothelial or submesothelial layers of peritoneum. These tumors may report as simple abdominal discomfort, abdominal distention, abdominal pain or palpable mass. Very rarely these peritoneal tumors can be included in differential diagnosis in patients presenting with diffuse or focal peritoneal disease.
So far only one case of a torted pedunculated abdominal wall lipoma mimicking acute appendicitis has been reported [7]. Another case of pedunculated lipoma presenting as abdominal pain, nausea and constipation which was diagnosed on diagnostic laparotomy was reported by Barut et al. [8].
Lipoma on USG appears as iso- to hyperechoic texture surrounded by thin, echogenic capsule. Computed tomography is reliable on diagnosis of deep lipomas, which appears as a well-circumscribed mass with uniform fat attenuation. However, in our case, diagnosis was made on diagnostic laparoscopy. Finding of macroscopically normal appendix during operation needs examination of other organs and parietal peritoneum. Though a rare case it should be kept in mind for a differential diagnosis of an acute abdomen. This benign neoplasm should be treated with total excision.

{kind=link}
{kind=link}
{kind=link}
{kind=link}