





Abstract
Glomus tumors (GTs) are benign tumors originating from the glomus body which are usually solitary and small lesions. The vast majority are found in the distal extremities, particularly in the hand, wrist, foot and under the fingernails rarely involving visceral organs. Here we report a rare case of gastric GT presented to us with exsanguinating hematemesis and severe anemia. All the initial diagnostic tests were inconclusive. Contrast-enhanced computed tomography abdomen revealed a soft tissue density lesion within the first part of duodenum. Diagnostic laparotomy was planned and a mass of 3 × 2.5 × 2 cm was found at pylorus along greater curvature, without any evidence of lymphadenopathy or metastasis. Distal gastrectomy with gastrojejunostomy was done. Histopathology confirmed the diagnosis of a GT. Immunohistochemistry of tumor cells demonstrated smooth muscle actin and CD34 (very focal).
INTRODUCTION
Glomus tumor (GT) is a rare, benign mesenchymal neoplasm arising from glomus body (dermal arteriovenous shunt responsible for skin thermoregulation) [1–3]. GTs are usually small, solitary lesions. Approximately 2% of all soft tissue tumors [1] commonly noted in the subungual finger extremities and rarely involving visceral organs. Preoperative diagnosis is difficult. GT generally presents with gastrointestinal (GI) bleed either hematemesis, malena or both. In this case we are presenting a rare case of gastric GT.
CASE REPORT
A 40-year-old female presented to her primary care physician with complaints of malena and hematemesis for 1 month. The patient also complained of mild respiratory distress, although her hemodynamic parameters were stable.
On examination she had pallor and mild splenomegaly. Her abdomen was otherwise soft, non-distended, without any palpable mass. Lymphadenopathy was not observed.
Apart from severe anemia (hemoglobin −2.5) and mild leucocytosis other laboratory parameters were normal. Ultrasonography demonstrated a well-defined mass in relation to the gastric pylorus. Upper GI endoscopy revealed an extrinsic bulge at D1 with normal overlying mucosa. Contrast-enhanced computed tomography abdomen showed a well-defined polypoidal soft tissue density lesion of size 36 × 29 × 30 mm seen within the first part of duodenum without exophytic component. Adjacent fat planes were clear. The differential diagnosis involved mesenchymal and other benign GI stromal tumors.
The patient was taken to the operative room electively after correcting the anemic status. She was subjected to distal gastrectomy with gastrojejunostomy. The stomach contained a 3 × 2.5 × 2 cm well-circumscribed tumor with normal overlying mucosa (Figs 1 and 2). Cut surface of the specimen, demonstrated a yellowish-white homogenous tumor, arising from the submucosa and infiltrating muscularis propria of the stomach, without involving the serosal surface. Histologically, the tumor cells are seen in sheets with intervening thin vascular septa. The cells have a uniform round nucleus and scant cytoplasm, without nuclear pleomorphism and no mitotic figures. Immunohistochemically, the tumor cells express smooth muscle actin, CD34 (very focal) and are immune negative for desmin, CD31, S-100 protein, synaptophysin, chromogranin A, HMB 45, c-kit and DOG-1. The proximal and distal cut margins are uninvolved. The patient recovered uneventfully and was discharged 7 days after surgery.
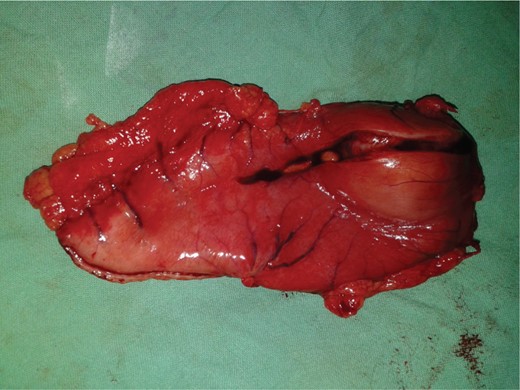
Postoperative resected specimen.
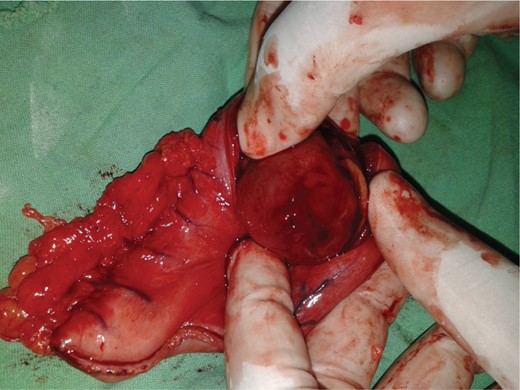
Postoperative resected specimen.
DISCUSSION
A GT is a rare benign neoplasm arising from the glomus body. Glomus body (or glomus apparatus) is a component of the dermis of the skin involved in body temperature regulation. The glomus apparatus consists of three vascular components: an afferent artery separated from an efferent venule by convoluted channels [4]. GTs are commonly observed in the extremities and are rarely found in visceral organs, but they have also been described in the bone and joints, skeletal muscle, soft tissue, tympanum, mediastinum, trachea, kidney, uterus and vagina [1].
The first case of gastric GT was reported in 1951 by Key et al. [5] and since then, few cases have been reported.
Gastric GT is a benign mesenchymal neoplasm arising from the neuromyoarterial glomus [4]. According to Miettin
en et al. [2], the frequency of gastric GTs is estimated to be 1% with that of GI stromal tumors. Gastric GT is far more common in women than in men. The tumor is usually solitary but cases of multiple gastric GTs have been reported.
Glomangiomas are submucosal masses that can remain asymptomatic and can be discovered incidentally or they may grow large enough to ulcerate the overlying mucosa and cause upper GI bleeding, melena and severe anemia.
A diagnosis by either esophagogastroduodenoscopy or upper GI series is difficult and an endoscopic biopsy is usually not helpful due to the intramural nature of the tumors.
Endoscopic ultrasound (EUS) can suggest the layer of origin of tumor but findings are insufficient to establish a diagnosis of GT, though EUS-guided fine-needle aspiration cytology can prove as an efficient diagnostic tool [3, 6, 7].
Histologically, GTs are well circumscribed and located in gastric submucosa or muscularis and comprise glomus cells surrounding capillaries. The glomus cells are small, uniform and round without nuclear pleomorphism, mitotic figures or necrosis.
Immunohistochemical staining showed positivity for smooth muscle actinin, vimentin and actin, calponin, type IV collagen and laminin.
Treatment of choice should be wedge resection with negative margins [4, 8]. Distal gastrectomy with reconstruction can be considered in tumors located in the pyloric region. Endoscopic submucosal enucleation reported to be a treatment option in many studies but with variable results [4, 9, 10].
CONFLICT OF INTEREST
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}