





Abstract
Gallstone disease is a common surgical presentation, and laparoscopic cholecystectomy is the favoured method of surgical management. Ligation of the cystic duct is usually performed with surgical clips, which have the potential to migrate into the common bile duct with time. This paper describes a case of cholangitis secondary to clip migration in a 42-year-old male patient 9 years after the initial laparoscopic cholecystectomy. Magnetic resonance cholangiopancreaography imaging revealed a surgical clip lodged in dilated common bile duct. The patient was managed successfully by endoscopic retrograde cholangiopancreatography.
INTRODUCTION
Gallstone disease is a common presentation in secondary care, and laparoscopic cholecystectomy is the most commonly used procedure for this condition with >60 000 procedures being carried out per year in the NHS.
Surgical clip migration following cholecystectomy is a rare but well-documented complication. The timeframe between the initial cholecystectomy and development of complications can be variable with case reports describing migration after as much as 14 years [1].
In most reported cases, the migrated surgical clip acts as a nidus for choledocholithiasis and subsequent biliary obstruction [2]. The exact pathophysiological process by which this occurs is not clearly understood but is thought to involve involution of the cystic duct with the attached clip into the lumen of the common bile duct as a consequence of compression by local structures, such as the liver [3]. Complete inversion and necrosis of the involuted duct then leaves the surgical clips free within the lumen of the common bile duct with subsequent complication such as obstructive jaundice, cholangitis, biliary colic or pancreatitis [4]. Most cases are treated successfully by endoscopic retrograde cholangiopancreatography (ERCP). This case report describes a patient who developed cholangitis secondary to surgical clip migration 9 years after the initial laparoscopic cholecystectomy.
CASE REPORT
A 42-year-old male with a history of cerebral palsy, learning difficulties and epilepsy was admitted with a 24-h history of nausea, vomiting and abdominal pain. Past surgical history included laparoscopic cholecystectomy with operative cholangiogram 9 years previously and laparotomy and drainage of a pancreatic pseudocyst 16 years previously.
Examination revealed a midline laparotomy scar and a distended, tender abdomen.
Laboratory tests revealed elevated liver function tests: ALP 285 U/l, ALT 465 U/l, GGT 669 U/l with a normal bilirubin. Magnetic resonance cholangiopancreatography demonstrated marked dilatation of the common bile duct to 15 mm (Fig. 1). A surgical clip was noted in the distal common bile duct, presumed to have migrated from the cystic duct, which it had been used to close 9 years previously.
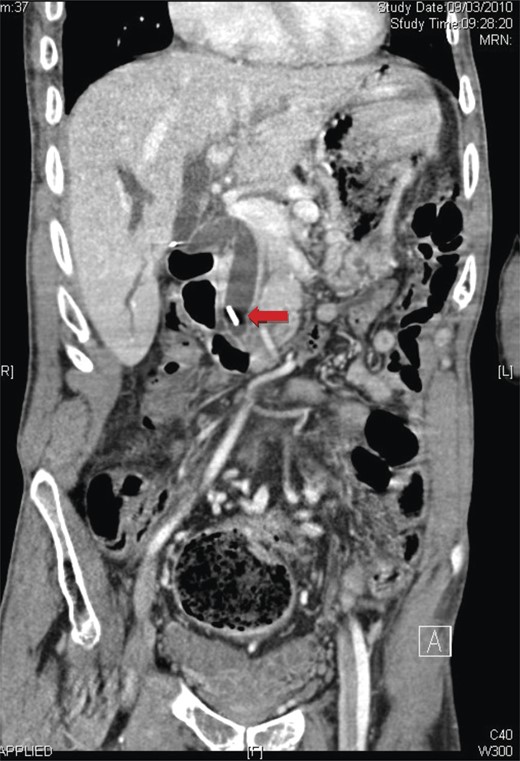
A coronal view of magnetic resonance cholangiopancreatography showing the presence of a surgical clip and common bile duct dilatation.
The patient had an ERCP and sphincterotomy during which the clip was removed leading to complete resolution of symptoms and return of biochemical markers to normal.
DISCUSSION
Although a rare complication of laparoscopic cholecystectomy, surgical clip migration is a well-documented event with several case reports published.
The mechanism by which surgical clip migration takes place is unclear but is thought to be partly affected by technical factors such as correct placement and use of minimal numbers of clips [5].
A proposed mechanism of clip migration by Kitamura et al. [3] initially involves the compression of the clipped cystic duct by the liver. The cystic duct and clips then become inverted into the lumen of the common bile duct. Over time, this structure becomes necrotic, and the clips fall away into the common bile duct where they can then act as a nidus for gallstone formation.
The time scale for this pathophysiological process can vary. Indeed, the time period between cholecystectomy and development of complications has been reported by Chong et al. [4] to be anything from 11 days to 20 years with a median of 26 months. The most common diagnoses at presentation are obstructive jaundice (37.7%), cholangitis (27.5%), biliary colic (18.8%) and acute pancreatitis (8.7%) [4]. The majority of cases are treated successfully with ERCP (77%) or surgery (20.2%) [4].

{kind=link}
{kind=link}