





Abstract
A 70-year-old woman presented with a short history of a spontaneous enterocutaneos fistula in the left inguinal region. A laparotomy revealed a fistulizing Richter's hernia. The fistulizing small bowel segment was resected and the femoral hernia repaired from below. Although rare, a complicating Richter's hernia should be considered in the differential diagnosis of a groin fistula.
INTRODUCTION
Richter's hernia is a strangulated hernia in which a portion of the circumference of the small intestine is trapped, which may become ischaemic but without the development of intestinal obstruction [1]. With bone (body of pubis medially) or ligament on three sides [inguinal ligament anteriorly, pectineal ligament of Astley Cooper on superior ramus of pubic bone posteriorly and the crescenteric edge of the lacunar (Gimbernat's) ligament medially], the femoral canal is a rigid opening so that bowel is more likely to become strangled if it is pushed through it [2]. There have been reports of Richter's hernia with strangulation in inguinal, femoral, incisional and port hernias after laparoscopic surgery [1, 3–5]. The formation of an enterocutaneous fistula following an incarcerated femoral hernia has, however, rarely been reported [6].
CASE REPORT
A 70-year-old widow presented with a week history of faecal discharge through the groin. This followed a groin abscess of a few days duration which spontaneously discharged. The faecal discharge and soiling was exacerbated by meals, but she did not have an altered bowel habit nor did she strain at stool. She had no abdominal pain, fever, anorexia and weight loss. She felt generally well except for the discomfort from the faecal soiling. She is a known human immunodeficiency virus (HIV)-infected patient and has been on antiretroviral treatment for the past 3 years but non-compliant. Her CD4 count was 144 cells/µl (<200 indicating AIDS). Three years ago, she had an incision and drainage of a left groin abscess with apparently no further complications. On examination, she appeared physically well but for a painless faecally discharging wound in the left mid-inguinal point at the groin crease (Fig. 1). There was no evidence of an underlying collection or abscess. The inguinal and femoral orifices appeared normal with no palpable lump or expansile cough impulse, although cough impulses are difficult to detect in femoral hernias. Peripheral pulses were normal. The rest of abdominal including rectal, cardiovascular and respiratory examinations were unremarkable. Her haemoglobin level was 11.6 g/dl (normal: 12.0–15.0) and her serum biochemistry was within normal limits. She had an abnormal clotting time probably consistent with the thrombocytopenia of HIV/AIDS. The differential diagnosis included a colocutaneous fistula from sigmoid diverticular disease in view of the faeculent and low output nature of the fistula and previous groin abscess or a perforating colonic carcinoma. A mid-line suprapubic incision revealed a loop of small intestine (ileum) protruding below the inguinal ligament to the femoral canal and grossly adherent to the external opening in the groin. Dissection of the adhesions surrounding the fistula was facilitated by a counter groin dissection of the fistula off the tight femoral ring defect (Fig. 2). Because of the localized and confined nature of the fistula in the ante-mesenteric border, a wedge excision was carried out and repair effected within the transverse axis by two layers of an absorbable (3-0 vicryl) suture (Fig. 3). The femoral canal was repaired from below by placing non-absorbable (2-0 nylon) sutures between the inguinal ligament and fascia over pectineus muscles with care being taken not to injure or compress the femoral vein lying laterally within the femoral sheath. Haemostasis was slow and difficult as expected from her bleeding diathesis and secured by patient packing. A mass closure of the abdominal wound with 1-0 nylon was followed by closure of the inguinal wound. Her postoperative haemoglobin level was 5.9 g/l for which she received 2 units of blood. Her bowels moved on Day 3, but subsequently deteriorated with abdominal distension and vomiting. She remained apyrexial, but gradually became hypotensive and died on the 12th postoperative day. No postmortem was done.

Spontaneous enterocutaneous fistula.
![Large fistula delivered into the abdomen via groin incision below [fistula in the ante-mesenteric border of the protruding loop of ileum].](https://oupdevcdn.silverchair-staging.com/oup/backfile/Content_public/Journal/jscr/2014/11/10.1093_jscr_rju121/2/m_rju12102.jpeg?Expires=1785948485&Signature=bvxmN6V1yvF1K0-neWdqhmz0a~blH24ZdL-WEdr7FEippi0oMGd76l6Jzi3PuPO5aMdwF4bD4np9lPLOfugEFgIY4zA4romGSMWgcclycWz7~H438-DyOqlX31PByEGefJHCgcCPzpEMmY01oeESI6dh3JnkK80SbY3AHkRFd95RmHWbbnm3kSfKLl~fwfrithASJ~ygCDqSYI-mwLGViGdea~R~wbOMls7qhW~K-be5C~DUgZlIMhQdwsjCza5V-UXZTm4cnlkFl-3Ob8qkA-08JJZGB3ReSLUSlB3vsISFPGDbsvj7BCHA-BPQJyFoZdUjxeCtA0vjy7itn3I5fg__&Key-Pair-Id=APKAIYYTVHKX7JZB5EAA)
Large fistula delivered into the abdomen via groin incision below [fistula in the ante-mesenteric border of the protruding loop of ileum].
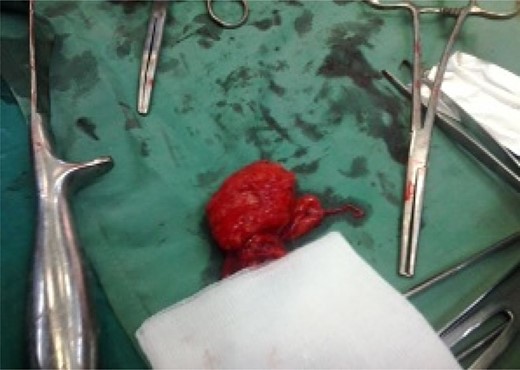
Wedge-excised fistulous segment.
DISCUSSION
Richter's hernia is dangerous because peritonitis can occur without previous obstructive symptoms. Femoral hernias account for 7% of all hernias and are four times more common in women than men because of the shape of the female pelvis and the loss of fat in the canal in elderly women [2, 6]. Twenty percent present with strangulation, but the hernia may easily be missed on clinical examination if the diagnosis is not thought of [1]. The left groin abscess that occurred in this patient 3 years previously was most likely a complicating Richter's femoral hernia, which had now recurred and progressed to an enterocutaneous fistula. An untreated Richter's hernia may lead to the formation of an abscess without communication to the peritoneal cavity with the secondary formation of an enterocutaneous fistula [6]. A preoperative diagnosis would have been determined by a computed tomography (CT) scan in resourced areas [3–6]. Surgically, a ‘high’ approach gives more generous access than does the ‘low’ (Lockwood) approach and is considered the better procedure when strangulation of femoral hernia has occurred or when an intra-abdominal pathology was suspected as in this case. It allows the hernia sac and its contents to be assessed and dealt with more easily at its highest point and renders direct access to and obliteration of the femoral ring [2]. In this case, a counter groin incision was made to facilitate the delivery and resection of the fistula abdominally, and the repair of the canal made easily from below. Postoperative complications would include wound haematoma/infection, recurrence which is very rare and lymphatic leak [2]. General anaesthesia may result in depression of cell-mediated immunity and AIDS progression (Table 1) [7]. Preoperative platelet transfusion would have been of benefit to this patient [8]. The fashioning of a stoma may have been preferable in this severely immunosuppressed patient, although the decision to raise a stoma could not be undertaken lightly in our setting [7, 8]. The closure of the small bowel defect may have contributed to the patient's death from sepsis [9]. In conclusion, a fistulizing Richter's hernia should always be considered as a differential diagnosis of an enterocutaneous fistula in the groin.
Centre for Disease Control—1993 revised classification system for HIV infection [9]
| Asymptomatic primary infection or Persistent generalised lymphadenopathy | Symptomatic (not A or C) conditions | AIDS, i.e. indicator conditions present | |
|---|---|---|---|
| 1. >500 CD4 cells/µl | A1 | B1 | C1 |
| 2. 200–499 CD4 cells/µl | A2 | B2 | C2 |
| 3. <200 CD4 cells/µl | A3 | B3 | C3 |
Written informed consent was obtained from the next of kin to the deceased for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor of this journal.
AUTHORS' CONTRIBUTION
E.P.W. is the main author and surgeon. M.P. provided primary medical treatment prior to referral and gave medical advice in the management. A.M.C. rendered advice and support on the orientation and literature search.
CONFLICT OF INTEREST STATEMENT
None declared.
ACKNOWLEDGEMENT
We thank the next of kin to the deceased for giving us consent to publish this case report, the medical student, Saquinatou Hamadjoda, for providing the images, and the theatre and surgical nursing staff of the Regional Hospital Buea for their perioperative care of the patient.

{kind=link}
{kind=link}
{kind=link}