





Abstract
Cecal masses secondary to extra-luminal compression are rare. We report a case of a 72-year-old man with a cecal mass found during routine colonoscopy with multiple biopsies showing normal colonic mucosa. The patient had a relevant past surgical history of a bilateral open inguinal hernia repair using the ‘Plug-and-Patch’ mesh system. A computed tomography scan of the abdomen and pelvis showed a 4 × 3.3 cm mass that compressed the wall of the cecum. A neoplastic process could not be ruled out. Diagnostic laparoscopy with intraoperative colonoscopy showed that the right hernia plug was not deployed and was causing extrinsic compression of the anterior cecal wall and an intraluminal impression upon insufflation of the colon. This case report reiterates the importance of combining intraoperative colonoscopy with laparoscopy for diagnosis of undetermined colonic masses.
INTRODUCTION
Inguinal hernias are common abdominal wall defects that can be repaired using the ‘Plug-and-Patch’ mesh system. Mesh migration is a long-term complication in open or laparoscopic procedures. Several case reports describe migration of the mesh to the cecum [1], colon [2], small bowel [3], bladder [1, 4], scrotum [5] and ovaries [6]. Mesh migration manifests clinically by obstruction, erosion, perforation or in rare cases, by mimicking malignancies [1–4, 6–9]. We report a case of an inguinal hernia mesh plug that mimicked a cecal mass, without migrating from the inguinal canal.
CASE REPORT
A 72-year-old man was referred for resection of a cecal mass that was found on routine colonoscopy (Fig. 1). The patient denied history of blood per rectum, change in bowel habits, abdominal pain, nausea or weight loss. The patient had a significant past medical history for prostate cancer for which he underwent prostatectomy and chemo-radiation therapy. He also underwent open repair of bilateral inguinal hernias in the remote past; the operative notes were not available to us. Tumor markers (CEA and CA19-9) and routine blood tests were unremarkable.

Colonoscopy: view of the cecum; a broad-based mass is present in the right lower corner of the photo. The mucosa appears normal and did not exhibit erythema or ulcerations.
The mass was found in the cecum during routine colonoscopy (Fig. 1); it had raised borders, did not have a stalk and was not associated with mucosal erythema or ulceration. Biopsies showed normal colonic mucosa. A computed tomography (CT) scan of the abdomen showed a 3.3 × 4 cm mass that compressed the wall of the cecum. There was no associated lymphandenopathy or liver lesions (Fig. 2). Based on these findings, we could not conclude if the aforementioned mass was intramural or extramural to the cecum. Due to the uncertainty about the location of this mass (intramural versus extramural) and the inability to rule out a neoplasm, we proceeded with a diagnostic laparoscopy with the possibility of resection of the cecum. Intraoperatively, we found that the right inguinal hernia had been repaired using a plug-and-patch technique. The mesh plug was fixed in the preperitoneal space and had not violated the peritoneal layer. The ‘Plug’ had not fully deployed in the preperitoneal space and had retained a cone-like shape. The wall of the cecum appeared normal and there were no masses in its anterior wall. An intraoperative colonoscopy was done to confirm the absence of a mass; upon insufflation of the colon, it became apparent that the cecal wall was pressed against the non-deployed plug thereby creating the impression of a mass with extrinsic compression.
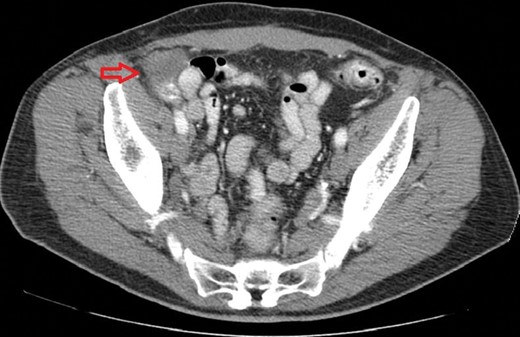
CT scan of the abdomen with intravenous and oral contrast demonstrating a mass in the right lower quadrant adjacent to the cecum.
DISCUSSION
This is a unique case of a non-deployed plug mimicking a cecal wall mass. We postulate that insufflation with air needed during colonoscopy abutted the distended cecal wall against the rigid mesh plug that maintained a conical shape, pointing towards the anterior wall of the cecum.
A very limited number of cases of bowel-related complications secondary to the ‘Plug-and-Patch’ mesh system have been reported in the literature [7]. Halm et al. [10] highlighted the increased incidence of synthetic mesh-related complications, such as mesh erosion into the small bowel, when placed intraperitoneally (8%) versus preperitoneally (0%). Given that the plug had not violated the peritoneum and was encased in a fibrous tissue layer, we opted not to remove the mesh plug because it did not pose an imminent risk of erosion. Also, the mass effect was situational and was the result of cecal distention during routine colonoscopy.
A non-deployed mesh mimicked a mass in the wall of the cecum; therefore, combining intraoperative colonoscopy and laparoscopy can be diagnostic to avoid an unnecessary resection of the colon.
CONFLICT OF INTEREST STATEMENT
Murr: Covidien (Consultancy, Unrestricted educational grant). All other authors report no conflict of interest.

{kind=link}
{kind=link}