





Abstract
Kirschner (K) wires can easily migrate, resulting in serious complications. We report a 49-year-old woman who had a rare and late complication related to the migration of K wire. It had been used for left hip replacement 8 years ago. The patient admitted to our hospital with breathing-dependent chest pain and increasing dyspnea for ∼2 h. Chest X-ray and chest computed tomographic scans revealed the presence of a metallic image of ∼5–6 cm in the right hemithorax. There was a large hemothorax but no pneumothorax. A right thoracotomy was performed and the wire was removed without complications. Surprisingly, no injury was noted to any intervening abdominal structure intra-operatively. Patients, who are treated with K wire, should be informed of the risk of wire migration and should undergo regular postoperative follow-ups including radiography.
INTRODUCTION
The migration of various internal fixation devices, especially Kirshner (K) wire, is well established. The wires usually follow a retrograde path, protruding near the entry point. When they migrate in the other direction, serious problems may occur. Migration of K wires from the upper extremity joints to intrathoracic cavity has been reported, but it is less common from the lower extremities [1, 2].
We describe an even rarer case where the wire migrated from the left hip to the abdomen perforating the right thoracic cavity and hemidiaphragm. The patient was treated successfully with open surgery.
CASE REPORT
A 49-year-old woman admitted to our hospital complaining of breathing-dependent chest pain and dyspnea with progressive onset lasting for 2 h. The pain was acute at onset, sharp in nature, worse on deep inspiration, did not radiate and was not reproducible with palpation. A day before presenting to us, she was admitted to another emergency unit with an acute pain in the right abdomen. Her symptoms had been interpreted as dyspepsia and she was discharged from the hospital with simple treatment.
The most remarkable of her past medical history was that she had been undergone total hip replacement 8 years ago at another institution. Previous pelvic radiograms of that period were not available.
On presentation, the patient was in mild respiratory distress with a respiratory rate of 30 breaths per min, heart rate of 90 bpm and oxygen saturation measured via pulse oximetry of 93% on room air. A respiratory examination revealed that right-sided findings of reduced chest expansion, diminished breath sounds and dullness in the lower right chest were found.
Laboratory investigations were within normal limits. The ECG was unremarkable. Chest X-ray showed the presence of a metallic image ∼5–6 cm long, located in the right hemithorax. There was a large hemothorax but no pneumothorax (Fig. 1). The investigation was complemented by a chest computed tomography (CT) that confirmed the presence of a metallic wire in the right pleural space.
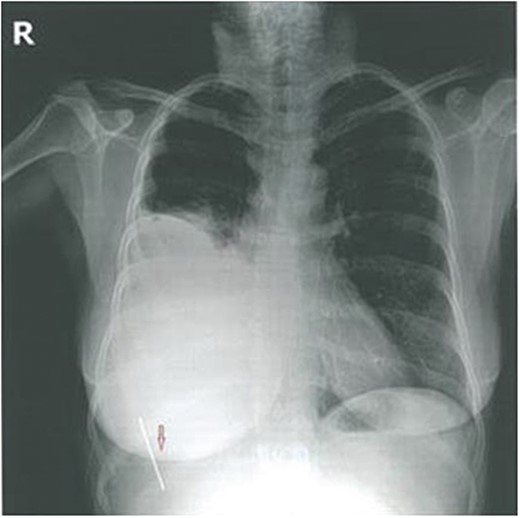
Preoperative X-ray.
Taking into account the hemodynamic state of the patient, her physical examination, the laboratory results and the CT-scan findings, we decided to perform an urgent surgical removal of the K wire under general anesthesia.
She was placed in a left lateral decubitus position and a posterolateral thoracotomy in the fifth right intercostal space was used. The wire was removed without complications. Surprisingly, no injury was noted to any intervening abdominal structure intra-operatively. As a precaution, a 28-F chest tube was placed. There was no air leak or bleeding postoperatively and the tube was removed on the second postoperative day. The postoperative outcome was favorable and the patient was discharged on postoperative Day 4 with a normal chest radiogram (Fig. 2).
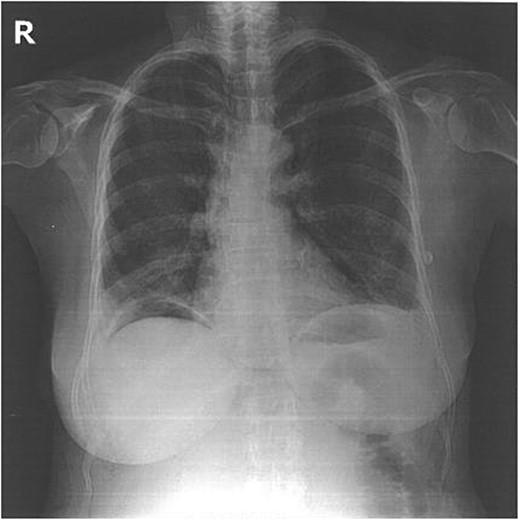
Postoperative X-ray.
DISCUSSION
The use of K wires is a common and standard practise. Intrathoracic migration of a K wire is a rare complication and is most commonly associated with its use in the surgical fixation of sternoclavicular and acromioclavicular joint dislocations [1–3]. Abdominal and pelvic migration of wires arising from the hip is well known too [4, 5]. We found a few reports of migration from the lower extremity into the heart [6–8].
We describe an even rarer case where a K wire migrated from the left lower extremity into the right thoracic cavity. The interesting point about our case is the long distance of the migration path of >1 m through which the wire passed through the hip joint and reached the abdominal cavity; the patient complained of an acute pain in the right abdomen during that time. When the K wire reached the intrathoracic cavity, she presented to the emergency department with worsening dyspnea and chest pain.
Migration of K wires has been reported as early as the first day and as late as 21 years [9] after the fixation. Usually, the process causes no symptoms, but there have been observed deaths attributable to migration. All deaths were associated with catastrophic cardiovascular events and cardiac tamponade. Serious, non-fatal complications include pericardial tamponade, arrhythmia, pericarditis, pseudo-aneurysm, aortopulmonary fistula, pneumothorax, hemothorax, hemoptysis, subclavian steal syndrome, hemianopia, hemiplegia, paraplegia, radicularpain, dysphagia and splenic hematoma [9, 10]. Our case had hemothorax and severe dyspnea.
Once intrathoracic migration of a K wire is recognized, urgent removal is mandatory. Video-assisted thoracoscopy, thoracotomy and sternotomy are safe and could be used to remove migrated wires [3]. In this case, the migrated wire was removed by thoracotomy. Her postoperative course was uneventful.
Patients who have a medical history of K wire fixation surgery of any part of the body present with respiratory or cardiac complaint, pneumothorax or hemothorax at any time, the possibility of wire migration should be considered and a thorough work-up should be done to investigate this. In addition, these patients should be informed of the risk of wire migration and close follow-up should be done both clinically and radiographically, until all the wires are removed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}