





Abstract
Clavicular tuberculosis is a rare entity, an unusual case of skeletal tuberculosis. We report a case of rare presentation of clavicular tuberculosis as a non-healing ulcer in the medial two-third and lateral one-third of the clavicle. The clinical picture was confusing because of the development of foul-smelling discharge due to secondary infection. The diagnosis is rarely suspected before biopsies because tumours are much more frequent than infections in this bone. With worldwide resurgence of tuberculosis, clinicians should maintain a high index of suspicion as more infection at unusual sites is being reported.
INTRODUCTION
Isolated tuberculosis (TB) of the clavicle with absence of involvement of neighbouring joint is rare [1]. With the re-emergence of TB as an important infection worldwide, more and more cases are being reported with unusual features. The clavicle is an uncommon site of skeletal TB. TB of the sternoclavicular region constitutes ∼1–2%, of all peripheral TB cases, of which spinal TB represents 50% of these lesions. Extrapulmonary TB is uncommon in the USA, and skeletal involvement accounts for 1–2% of all cases of TB and ∼10% of extrapulmonary TB [2]. Due to its peculiar blood supply, extra pulmonary TB in the sternoclavicular region is quite uncommon [3]. The tubercular presentation at this site may frequently be atypical, leading to diagnostic confusion and to delays in appropriate therapy. In the few reports available, the lateral end of the clavicle has been found to be less frequently diseased than the medial end [4]. Additionally, TB has been known to mimic all types of lesions. Isolated clavicular lesion without associated pulmonary lesion creates a diagnostic dilemma. A recent case report highlighted a case of TB of the ascending colon [5] and in the medial end of the clavicle in a patient undergoing dialysis [2].
CASE REPORT
A 35-year-old male presented to us with ulcerative lesion over the right shoulder region for 2 years. The lesion was gradually progressive, which later developed a foul-smelling discharge. For this complain, he visited various physicians and was prescribed various antibiotics but there was no relief of complain. There was no history of trauma, cough, pain chest, dyspnoea or fever. Past history was insignificant. There was no history of TB and no one in the family had a history of TB.
Clinical examination revealed an ulcerative lesion 3 × 2.5 × 2.5 cm in the right clavicle at the junction of medial two-third and lateral one-third of the clavicle, with irregular margins, firm base and foul-smelling discharge. Bone was seen exposed with sequestrum present (Fig. 1). There was no evidence of cervical or axillary lymphadenopathy and the lung fields were essentially clear. Routine investigations showed moderate hypochromic microcytic anaemia, haemoglobin 9 g/dl, total leukocyte count of 7900 with polymorphs 42%, lymphocytes 54% and eosinophil 4%. Renal and hepatic panels were within normal limit. ESR was 35 mm. The gram staining of the discharge from the ulcer revealed gram-positive cocci, and the Ziehl Nielsen staining for acid-fast bacilli was negative. Culture of the discharge revealed growth of Staphylococcus aureus. ELISA IgG/IgM for TB was negative. HIV-I and II were negative. Chest X-ray was grossly normal (Fig. 2). Sequestrectomy was done and the bone along with the excised tissue was sent for biopsy. Histopathology showed it to be either foreign body granuloma or rare possibility of tubercular pathology.

Arrow heads show ulcer at the time of presentation.
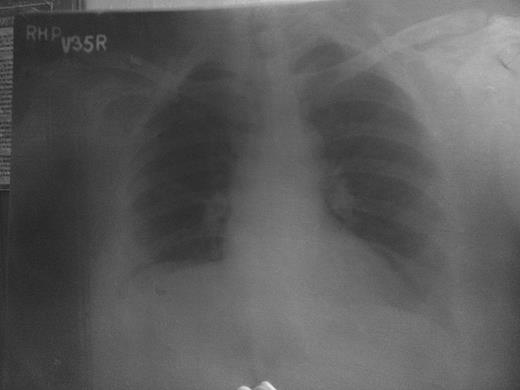
Pre-op X-ray chest PA view.
Patient put on Category I ATT. Patient responded to treatment. The ulcer over shoulder healed in 6 weeks (Fig. 3) with formation of granulation tissue. Patient completed full course of ATT and is doing well on regular follow-ups.

Arrow heads show ulcer after taking ATT with granulation tissue.
DISCUSSION
The occurrence of TB in the flat bones of chest and skull is very rare. With widespread knowledge and awareness of pulmonary TB, unusual sites are becoming a common cause of diagnostic dilemma [6]. However, cases of clavicular or sternoclavicular TB are few. The predilection yields are children, old people, poverty and immunodeficiency. It mostly locates in vertebrae, the hip and the knee. The clavicle localization is exceptional [7]. The diagnosis is rarely suspected before biopsies because tumours are much more frequent than infections in this bone. The lesions may be destructive or proliferative (spinaventosa). Plain radiographs may show diffuse thickening and honeycombing or multiple cystic cavities or sequestration, similar to pyogenic osteomyelitis. Radiography is not an effective means of evaluating changes in the clavicle because of overlapping anatomic structures. MRI is the investigation of choice [8]. It can show loss of normal hypodense cortices. If the diagnosis is quickly done, the treatment is medical: A combination of four antitubercular drugs during the initial 2 months, followed by a combination of 2 antitubercular drugs during 8–10 months. The response to the treatment is controlled clinically by the decreasing of the swelling or ulceration, and biologically by the decreasing ESR [9]. Surgical excision may be justified when the diagnosis is uncertain or the disease is unresponsive or for removal of a large sequestrum. A large part of the clavicle can be excised without loss of function [10]. To conclude, as to any chronic discharging sinus at an abnormal place not responding to routine treatment, a high index of suspicion should be kept for TB, especially in endemic areas.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}