





Abstract
At Bunbury Regional Hospital, we recently saw a case where Kirschner wires (K-wires), used during open reduction and internal fixation of olecranon, were propelled down the intramedullary canal intraoperatively. The K-wire was only secured unicortically. From our experience, we have developed steps to prevent this complication. First, where the wires are being used as part of a tension band wire construct, we suggest drilling the distal hole prior to the placement of the K-wires and, secondly, where K-wires are being used to secure the fracture fragment, the K-wires can be secured with artery clips to ensure that the wires remain in position.
INTRODUCTION
We present a case that occurred at Bunbury Hospital where a Kirschner wire (K-wire) has been propelled distally down the intramedullary canal of the ulna when it made contact with the drill. In both cases, the K-wires were only secured unicortically.
CASE STUDY
Ms R is a 68-year-old female who had a fall off a push bike and presented to the Emergency department with a comminuted fracture of the left olecranon. She was taken to theatre for an open reduction and internal fixation with a tension band wire construct. The fracture was reduced and held with two intramedullary K-wires. A hole was drilled in the proximal ulna to secure the cerclage wire distal to the fracture. During this process, the drill made contact with the K-wire and it was propelled distally within the intramedullary canal. On radiographic screening, the K-wire was sitting in the distal ulna. The wire was secured and removed with a set of artery clips (Fig. 1). Once removed, the fracture was re-reduced with two bicortical K-wires and a set of artery clips were used to secure them (Fig. 1).
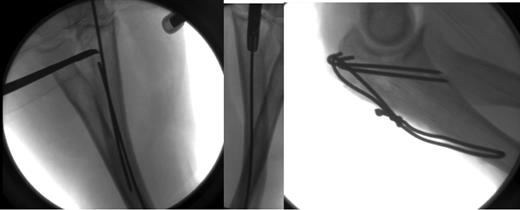
Left—K-wire secured and removed with a pair of artery clips. Right—Final shots of the Tension band wiring construct.
DISCUSSION
There is currently no published literature on avoiding intra-operative K-wires migration into the distal intramedullary canal of the ulna during olecranon open reduction and internal fixation. The literature on K-wire migration in the context of olecranon ORIF is limited to outward migration of the K-wires post-operatively [1–5]. There is also literature on post-operative intra-thoracic migration of K-wires post-clavicle ORIF [6]. In all cases, migration of the K-wire has been attributed to its smooth circular surface, which is prone to loose fixation on the surrounding bone. To prevent migration of the K-wires, different techniques were proposed by different authors. The rates of post-operative K-wire migration in olecranon tension band wiring are noted to be between 20 and 45% [1–3]. The techniques discussed in the literature are to prevent the K-wires from backing out post-operatively. In the context of upper extremity and thoracic trauma, Sharma et al. found that post-operative migration was eliminated through bending the end of the K-wire [6]. In this situation, with the K-wire being pushed into the distal ulna, bending the end would not be appropriate. In the first case, the cerclage wire needs to be positioned prior to bending. In the second case, where the K-wires are used to temporarily hold the fracture, it would make repositioning and removal of the wires difficult.
Some studies have delineated methods that can be employed to minimize the risk of intra-operative migration of the K-wire into the ulna. Larsen et al. suggested the use of non-sliding pins that have a sharp K-wire on one end and a bulb with a hole for the cerclage wire on the other end. The smaller diameter of the K-wire compared with the bulb stops it from migrating distally [4]. Non-sliding pins however are more expensive than standard K-wires and removing them, if required, is also technically more challenging. For these reasons, although good results have been produced since the mid-1980s, they are not widely used.
In both described instances of distal intra-operative migration of K-wires, the wires were inserted unicortically, within the ulna intramedullary canal. This technique was originally described by AO [7]. The modified technique of bi-cortical wire placement has shown benefits in terms of lower complication profile: with lower rates of wire migration-post-operatively and also improved stability [5, 8, 9]. Critics have argued that bi-cortical positioning of K-wires could cause iatrogenic damage to the ulna artery and the median nerve [7]. Cadaveric studies have demonstrated that this could be avoided by ensuring that the wire end does not protrude beyond the anterior ulnar cortex by >1 cm at a distance of 1.5 cm distal to the coronoid [7]. As well as offering superior biomechanical fixation, bi-cortical positioning of the K-wires offers greater resistance to migration of the wire both intra-operatively and post-operatively. It may be employed as a strategy to avoid the wire from migrating through the medullary canal of the ulna when the drill makes contact with it. It may, however, cause the wire to be propelled out of the ulna.
CONCLUSION
From our experience, we have developed steps to prevent this complication. Firstly, we suggest drilling the distal hole prior to placement of the K-wires. Secondly, the K-wires can be secured with artery clips to ensure that the wires remain in position. We have used these techniques successfully since the occurrence of these cases.

{kind=link}
{kind=link}