





Abstract
Meckel’s diverticulum (MD) is a common congenital anomaly, usually symptomatic in early childhood. The presence of multiple heterotopic tissues within a single diverticulum is rare and poses significant diagnostic challenges. In this report, a 12-year-old male presented with a month-long history of painless lower gastrointestinal (GI) bleeding (melena and hematochezia). While endoscopy was normal, 99mTc scintigraphy revealed MD in the right pelvic region. Laparoscopic diverticulectomy was performed, and histopathology confirmed MD containing dual ectopic gastric and pancreatic tissues. Symptoms resolved completely postoperatively. MD occurs in 2% of the population; while typically associated with gastric mucosa, the coexistence of pancreatic tissue is uncommon and can lead to atypical presentations in older children. This case underscores the value of the Meckel’s scan and clinical suspicion beyond early childhood. MD should be considered in adolescents with unexplained GI bleeding, as rare histopathological findings and prompt surgery are key to successful outcomes.
Introduction
Meckel’s diverticulum (MD) is the most prevalent congenital gastrointestinal (GI) anomaly, classically defined by the “rule of twos”: a 2% population prevalence, a 2:1 male predominance, and a location ~2 feet proximal to the ileocecal valve. While often associated with other systemic malformations, it lacks a definitive hereditary pattern. Although it can remain silent, the condition most frequently presents in early childhood, with a mean age of 2.5 years and the majority of symptomatic cases manifesting before the age of 2 [1]. The clinical manifestation of MD varies significantly with age. In pediatric patients, GI bleeding is the primary symptom. Conversely, symptomatic presentation in adults is rare and typically involves intestinal obstruction or diverticulitis. Due to this low clinical suspicion in adults, the condition is frequently misdiagnosed preoperatively [2].
The definitive management of symptomatic MD entails surgical intervention, including diverticulectomy, wedge resection, or segmental ileal resection. The choice of technique is dictated by the integrity of the diverticular base and the adjacent ileum, as well as the presence and distribution of ectopic mucosa within the diverticulum [3].
Case presentation
A 12-year-old male presented with a 1 month history of painless lower GI bleeding, occurring twice daily, manifesting as both melena and hematochezia. Physical examination revealed no fever, vomiting, constipation, diarrhea, or other signs of bleeding. The patient was alert and had good oral intake. Laboratory investigations were largely within normal limits, showing a hemoglobin level of 11.4 g/dl and a mean corpuscular volume of 78 fl.
Upper GI endoscopy with biopsies was conducted to exclude an upper GI source of bleeding and revealed no abnormal findings. 99mTc scintigraphy demonstrated a persistent abnormal focus of radiotracer uptake in the right pelvic region on serial imaging, consistent with the diagnosis of MD (Fig. 1).
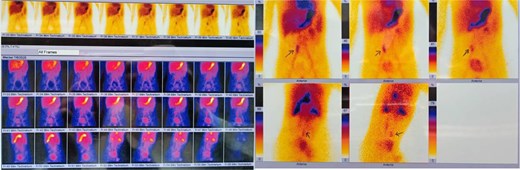
99mTc scintigraphy for detection of Meckel diverticulum.
Laparoscopic abdominal surgery was performed (Fig. 2), including diverticulectomy and end-to-end enterogastric anastomosis, by experienced surgeons. The patency and function of the anastomosis were confirmed intraoperatively. Histopathological examination of the diverticulum specimen revealed a small bowel segment consistent with MD, containing ectopic gastric and pancreatic tissue (Figs 3 and 4), with no neoplastic changes observed.

Intraoperative laparoscopic view of MD.
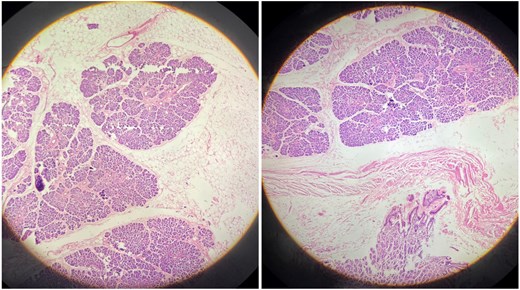
Histopathological examination (H&E stain) of the ectopic pancreatic tissue.
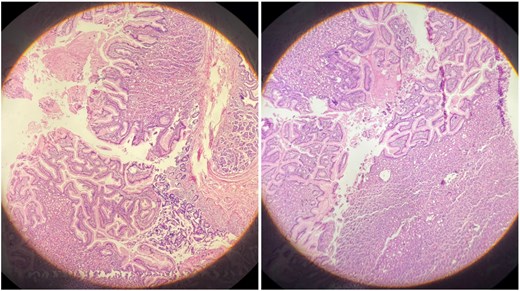
Histopathological examination (H&E stain) of the heterotopic gastric mucosa.
Postoperatively, the patient showed significant clinical improvement, with restored bowel function and no recurrence of bleeding, and was discharged in good condition.
Discussion
Meckel’s diverticulum is the most prevalent congenital anomaly of the small intestine, resulting from the incomplete obliteration of the vitelline (omphalomesenteric) duct. Occurring in ~2% of the population, it often remains asymptomatic, posing a significant diagnostic challenge in clinical practice [4–6].
Histologically, the ileal mucosa typically lines the MD; however, ectopic tissue is frequently present, particularly in symptomatic cases. Gastric tissue is the most prevalent, with a reported prevalence ranging from 4.6% to 71.0%, while pancreatic tissue is less frequent (0%–12.0%) [7], also the occurrence of several ectopic tissues within a single MD is not well documented in the literature and is relatively uncommon [6]. In this context, our case is of particular interest as the histopathological examination revealed the presence of both gastric and pancreatic heterotopic tissues, aligning with the rare clinical presentations described.
Although MD is typically discovered incidentally during abdominal investigations for unrelated conditions and often remains clinically silent, symptoms—when they occur—predominantly manifest in early childhood [8]. Supporting this clinical pattern, a series of 65 pediatric patients demonstrated a mean age at presentation of 3.2 years, with the vast majority of cases appearing before the age of 5 [9]. While these statistics underscore a predominant manifestation in early childhood, our case involving a 12-year-old male demonstrates that clinical presentation can extend into late childhood and early adolescence. This significant deviation from the typical mean age of 3.2 years highlights the critical necessity of maintaining a high index of clinical suspicion for MD across the entire pediatric spectrum.
The primary clinical manifestations of MD in the pediatric population include GI bleeding, abdominal pain, perforation, and intussusception [10]. Comparative studies between pediatric and adult cohorts further establish that lower GI bleeding is the predominant clinical hallmark in children, representing the classic symptomatic presentation [11]. However, our case presented a diagnostic challenge characterized by a mixed pattern of lower GI bleeding and melena. This atypical presentation deviates from the classic pediatric literature and underscores the clinical variability of the condition, which can complicate the initial diagnostic workup.
The diagnosis of MD remains challenging due to its non-specific clinical and radiological features. Conventional imaging, such as ultrasonography and CT, often fails to differentiate the diverticulum from normal bowel loops. Consequently, the 99mTc-pertechnetate scan remains the diagnostic gold standard, particularly in the pediatric population, where it demonstrates an accuracy exceeding 90% [12]. Regarding our patient, a 99mTc scintigraphy was performed on the abdominal and pelvic region, where sequential images demonstrated focal radiotracer uptake consistent with a MD located in the right pelvic region. An upper GI endoscopy with small bowel biopsies was also conducted for pathological evaluation. The histopathological examination confirmed a small bowel segment showing both ectopic gastric and pancreatic tissue, which is considered uncommon as said before.
The surgical management of MD is guided by several critical variables, including the size of the diverticulum and the presence of inflammation, perforation, or infection. While diverticulectomy is generally a simple laparoscopic procedure with a low complication rate, a formal small bowel resection may be required in cases involving bleeding or severe inflammation. This extensive approach is often necessary to guarantee the complete removal of all heterotopic mucosa, which is essential for preventing recurrence of symptoms [13]. Consistently, this surgical approach was successfully employed in our case, ensuring definitive treatment.
Conclusion
In conclusion, MD remains a diagnostic challenge when presenting atypically beyond early childhood. The rare coexistence of dual gastric and pancreatic ectopic tissues in this case underscores the condition’s histopathological variety. 99mTc scintigraphy and timely laparoscopic intervention proved essential for accurate diagnosis and definitive treatment. This case reinforces the need to maintain clinical suspicion for MD in any pediatric or adolescent patient with unexplained GI bleeding.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}