





Abstract
Orbital blowout fracture frequently occurs along the floor or medial aspect of the orbital wall, which are the two thinnest areas of the bony orbit. True trapdoor injury of the orbit is less common and is rare as an isolated medial wall injury, because the medial orbital wall has several bony septa within the ethmoid sinus that provide support and decrease the risk of a trapdoor fracture. Additionally, the incidence of trapdoor-type blowout fracture in adults is lower than in children. In a trapdoor-type blowout fracture with restricted ocular movement, prompt diagnosis and early intervention are associated with better clinical outcomes. We encountered a case of trap door-type medial blowout fracture with horizontal eye ball movement limitation in an adult. She underwent endonasal endoscopic reduction surgery for the medial blowout fractures. Here we report this case, and suggest early diagnosis and prompt surgical exploration.
INTRODUCTION
A blowout fracture is characterized by outward fracture of the orbital wall with ocular symptoms such as diplopia, eyeball movement restriction and enophthalmos of the invaded orbit. The white-eyed blowout fracture, first reported by Jordan et al. [1], is described as a trapdoor orbital floor fracture, linear and hinged in form, which allows herniation of the orbital contents through the fracture. The incidence of trapdoor-type medial blowout fracture is extremely low compared with that of floor one, and is easily missed due to the lack of other prominent soft tissue injury signs [2]. This type of blowout fracture has significant morbidity if left untreated. Here we describe a case of trapdoor-type medial blowout fracture with horizontal eye ball movement limitation that was treated via an endoscopic endonasal approach.
CASE REPORT
A 38-year-old woman presented diplopia with left lateral gaze after sustaining trauma to the left orbit. There was mild periorbital edema and ecchymosis at presentation. Ophthalmologic examination results were within normal except of ocular motility revealed an abduction deficit in the left eye (Fig. 1A). Computed tomography (CT) demonstrated a trapdoor-type left medial orbital wall fracture with entrapment of the medial rectus muscle (Fig. 2A). She was immediately taken to the operating room and underwent surgery under general anesthesia. Endoscopic endonasal reduction surgery for medial blowout fracture, first introduced by Yamaguchi [3] was used to expose the fractured medial orbital wall. The entrapped medial rectus muscle and herniated orbital tissue were gently released from the fracture after ethmoidectomy. The herniated orbital tissue and fractured bone were reduced to the original position, and then supported with a suitably sized Silastic sheet placed in the ethmoid sinus in an inverse U shape. A piece of Merocel® was packed between the Silastic sheets to provide support and prevent orbital tissue herniation, which were removed 4 weeks later at out-patients clinic (Fig. 3). The patient's ocular symptoms completely resolved 3 days postoperatively (Fig. 1B). Computed tomography scans demonstrated that the medial rectus muscle was reduced after surgery (Fig. 2B).
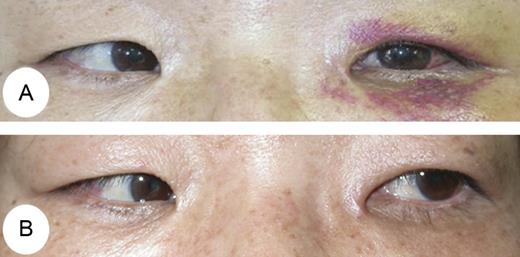
(A) Left ocular movements showed prominent limitation of abduction preoperatively. (B) After surgery, ocular movement was completely improved.
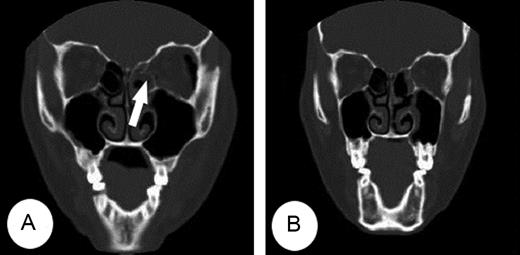
(A) CT showed a trapdoor fracture of the left medial orbital wall with the medial rectus muscle entrapped (arrow) within the fracture. (B) The entrapped medial rectus muscle and fractured medial wall were resolved on post-operative CT.
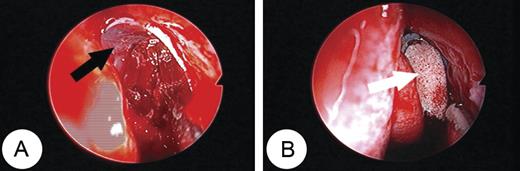
(A) A suitably sized Silastic sheet implant (black arrow) was inserted in an inverse U shape after assessment of ethmoid volume. (B) A piece of Merocel (white arrow) was packed between the Silastic sheets.
DISCUSSION
A blowout fracture is a common injury of the orbit and typically involves the thin bones of the medial wall and/or floor. Although the medial orbital wall is thinner than the floor, the floor is more susceptible to fracture because the floor has no central support. Conversely, the medial wall has many bony septa within the ethmoid sinus that support the wall and make deformation less likely [4, 5]. Thus, orbital fractures of the medial wall are reported, uncommonly. Some reported that most blowout fractures involved the orbital floor with only 4–12% involving the medial wall [1, 4]. The proposed mechanism of blowout fracture includes the hydraulic and buckling theories [4]. The trapdoor-type orbital fracture can be explained by buckling theory. Indeed, there is no real medial rim to transmit energy to medial wall, thus medial wall fractures are most likely purely hydraulic in nature, which may be an additional reason of low incidence trapdoor-type medial blowout fracture.
Jordan et al. [1] first described the ‘white-eyed blowout’ as an orbital floor fracture which is more commonly seen in children than adolescents. The bone in children is thought to be relatively thicker and more elastic, and when pressure increases within the orbit from a blow, the bones may crack and form a hinged trapdoor that is transiently displaced to the sinus. On release of orbital pressure, the trapdoor snaps back in position, entrapping the orbital tissue in the sinus [1]. It is presumed that medial orbital wall fractures occur in the same fashion. However, the medial wall has many supporting bony septa and it is uncommon to sustain a trapdoor-type fracture. Thus, to date, the majority of reports have been concerning trapdoor-type fractures of the orbital floor, whereas medial wall trapdoor-type fractures have been discussed relatively infrequently [6]. Additionally, an adult case of trapdoor-type medial blowout fracture has been reported uncommon [7].
The clinical presentation of medial blowout fractures includes horizontal diplopia, restricted abduction and limited adduction due to entrapment of the medial rectus muscle. Treatment guidelines for medial wall fractures are variable; classic indications for surgical intervention include severe oculocardiac reflex, entrapment of extra-ocular muscle, early enophthalmos and persistent dipolpia [8]. Many authors have demonstrated better clinical outcomes in trapdoor fractures of the floor when surgery is performed within days of the injury [7, 8]. We believe that trapdoor blowout fracture of medial wall acts similarly.
Yamaguchi et al. reported the first application of endoscopic intranasal reconstruction of the medial orbital wall [3]. High-resolution endoscopes and the advent of endoscopic instruments for sinus surgery now provide the surgeon with excellent endonasal visualization and access to the orbital walls without major complications [9]. Malhotra et al. [10] insist that endoscope-assisted orbital surgery provided magnified view with good visualization of the fractured structures of the medial orbital wall, good local illumination and allowing the trainee to safely perform selected complex orbital procedures. In this case, we surgically repaired the orbital medial wall fractures using an endoscopic endonasal approach with successful l results.
In conclusion, as with white-eyed blowout fracture, we recommend early surgical intervention and prompt surgical release of entrapped soft tissues, which can result in a complete resolution of symptoms for trapdoor medial wall fracture with rectus muscle entrapment in adults.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}