





Abstract
Intraperitoneal perforation can occur as a rare but life threatening complication of indwelling urethral catheters. Computed tomography (CT) revealed the bladder perforation by the Foley catheter. The injury could not be managed conservatively due to the presence of systemic infection. We present the case of a successful laparoscopic repair of the bladder due to indwelling urethral catheter.
INTRODUCTION
Intraperitoneal perforation is a rare and serious complication of indwelling urethral catheters. Bladder perforation should be included in the differential diagnosis, especially if patients are known to have an indwelling catheter. The laparoscopic approach is the best short recovery and less traumatic treatment for simple and accessible bladder injuries.
CASE PRESENTATION
A 73-year-old woman with a medical history of Parkinson's disease and chronic restrictive respiratory failure due to kyphoscoliosis was hospitalized for acute coronary syndrome. During hospitalisation, a bladder Foley catheter of size 16 French was placed for drainage and haemodynamic monitoring.
Forty-eight hours later, she presented with acute respiratory distress and septic shock requiring ventilatory assistance. She had no abdominal pain and no signs of peritoneal irritation. The daily diuresis was around 900 mL. The urinalysis was positive for nitrites, leukocytes and hematuria. Laboratory tests showed serum urea 10 mM/L and serum creatinine 232 µM/L. Plain radiographs of the abdomen did not reveal any signs of perforation or intestinal obstruction.
Together with vasoactive medication, intravenous antibiotics (Tazocilline and Linezolid) for nosocomial-acquired pneumonia were administrated. The patient showed no sign of haemodynamic improvement regardless of the antibiotic therapy.
Thoraco-abdomino-pelvic CT scan was then performed. The pelvic sagittal scan showed the Foley catheter perforated the urinary bladder and liquid effusion likely to be urine (Figure 1). The Foley catheter was unfortunately withdrawn to be well replaced.
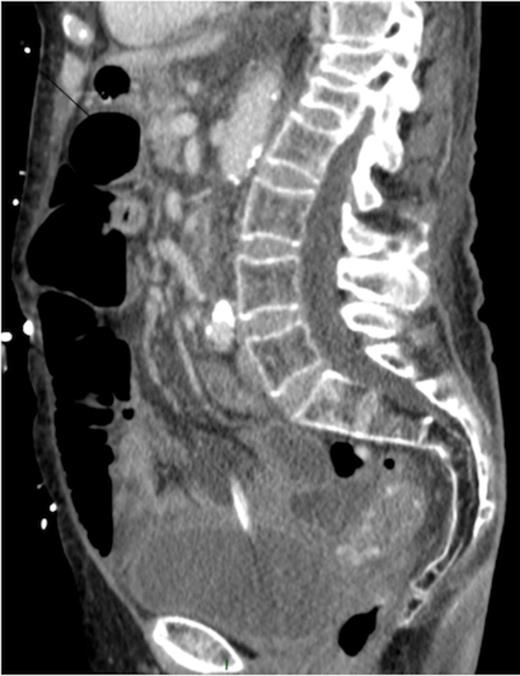
Sagittal CT image showing urethral catheter in the abdominal cavity.
Due to systemic infection with no sign of improvement, a laparoscopic surgical exploration was decided. The patient underwent laparoscopic surgery with three trocars, a 10 mm umbilical trocar and two 5 mm trocars, one in each iliac fossa. Abdominal exploration found bowel loops of the ileum clustered at the bladder and liquid in the peritoneal cavity. Despite adhesiolysis, the perforation was not visualized. Methylene blue dye was injected through the Foley catheter and it highlighted a 1 cm perforation in the bladder dome (Figure 2) with no other macroscopic lesions. The perforated part was sutured with interrupted vicryl in one layer. A methylene blue dye test was performed and excluded a leak. Abdominal cavity lavage with 0.9 % saline was performed. A suction drain was placed into the pouch of Douglas.

Methylene blue dye highlighting the bladder perforation
The patient's condition improved 24 hours after surgery allowing cessation of catecholamine and extubation. Renal function returned to normal with a good urine output from the Foley catheter. The Foley catheter was removed on day 15. The postoperative course was uncomplicated.
DISCUSSION
Laparoscopic repair of intraperitoneal bladder perforation was first described in 1994 and since then, a few cases of such approach have been reported to treat traumatic, spontaneous and iatrogenic bladder rupture, avoiding laparotomy (1). The laparoscopic approach is the best short recovery and less traumatic treatment allowing visualization of the entire peritoneal cavity to exclude others lesions.
Laparoscopy is a minimally invasive technique to treat abdominal trauma. It can avoid laparotomy in 63% of the cases, decreasing its associated morbidity (2). In the presence of simple and accessible injuries the therapeutic laparoscopy is performed.
Abdomino-pelvic CT scan is frequently performed in hospitalised patients and the bladder is included in the examination. In many cases the urinary bladder is catheterised for various indications. Familiarity with the different bladder pathologies and a routine meticulous search for them are indicated in every case. (3)
Early diagnosis and laparoscopic treatment might decrease the high mortality rate associated with this uncommon but treatable condition (4).
Aged patients with an acute abdomen might not complain of abdominal pain, and abdominal tenderness might be relatively mild (5). However, bladder perforation should be included in the differential diagnosis, especially if patients are known to have an indwelling catheter.

{kind=link}
{kind=link}