





Abstract
Squamous cell carcinoma (SCC) of urinary tract is a rarely encountered tumor. The incidence of this tumor is 1.4 per cent of all renal malignancies (1). We present a case of 52 years male with squamous cell carcinoma of renal pelvis, presenting as chronic pyelonephritis transforming the kidney into non-functioning multicystic cavitatory mass without any renal calculi. The case highlights the rarity of tumor in absence of calculi or any other predisposing factor. Moreover, histology of resected specimen detected features of SCC giving importance to careful and exhaustive assessment of specimen and of histologic sections, when there is no suspicion of malignancy clinically.
INTRODUCTION
Primary malignant tumors of renal pelvis are relatively rare and constitute about 8-14% of all renal malignancies (1). Urothelial carcinoma occurs in more than 90% of cases and SCC only in 0.7% to 7% (2).These tumors are mostly seen in adults and less commonly in pediatric age groups. Although the pelvic tumors are detected clinically at an early stage because of early desquamation of cells and hematuria, still the survival rate is not good enough. The common etiological factors include renal calculi, infections, endogenous and exogenous chemicals, vitamin A deficiency and hormonal imbalance, however, SCC have been reported even in the absence of these factors (3). The case being reported had SCC of renal pelvis presenting as hydronephrosis and chronic pyelonephritis in the absence of renal calculi and other predisposing factors. The tumor was diagnosed only after resection of the specimen and its extensive sampling.
CASE REPORT
A 52 years old male patient, farmer by occupation presented with complaints of heaviness and swelling in left side of upper abdomen since one year. The swelling was increasing in size gradually with occasional episodes of pain in left loin without radiation to any other side and occasional burning sensation during micturition. Routine haematological investigations, biochemical investigations and chest radiograph were normal. Urinary examination revealed microscopic haematuria.
Ultrasonography of abdomen showed grade-III hydronephrosis in left kidney with dilated pelvis and ureter. There was no free fluid and the right kidney was normal in size, shape and echotexture.
Intravenous Pyelography (IVP) showed prompt secretion of contrast by right kidney, which measured 14.4×5.9 cm with normal pelvicalyceal system. There was mild dilatation of renal calyces and right upper 2/3rd ureter. Left kidney and left ureter were not visualized up to 4hrs. Post micturition film showed adequate emptying.
Diethylene Triamine Penta-acetic Acid (DTPA) Scan revealed non-functioning left kidney with glomerular filtration rate (GFR) of 0.28 ml per minute per 1.73m2 with total GFR 61ml/min/1.73m2 (normal value: 64.8ml/min/1.73m2) and right kidney was normally functioning with GFR of 60.7 ml/min/1.73m2. A large photon deficient area was noticed in left renal fossa in the initial images. No significant tracer uptake was noticed in left kidney in the entire course of study till 4hrs.
The patient underwent nephrectomy for non-functioning kidney thought to be due to chronic pyelonephritis and the resected specimen was submitted for histopathology.
Gross examination of the specimen showed a multi-cystic sac-like structure measuring 11 x 6 x 2.5 cm along with the attached ureter. There was no visible renal tissue macroscopically. Cut surface of specimen showed multiple loculi with varied appearance and thinned out wall at some places with intervening thickened areas at others (Fig 1).
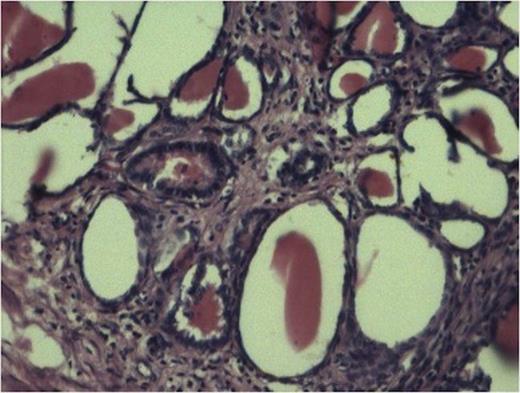
Tubules showing thyroidisation favouring chronic pylonephritis. (100x H and E stain).
The sections from various representative areas revealed dilated pelvicalyceal system lined by metaplastic squamous epithelium and shows changes of chronic pyelonephritis (Fig 2).
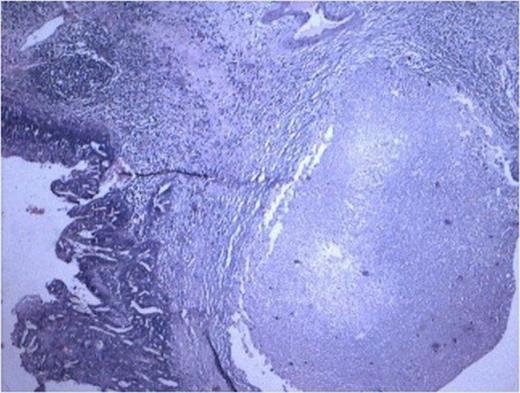
Cyst lined by metaplastic epithelium with focus of malignant squamous cell. (100x H and E stain)
Histopathology from solid portions in pelvis region showed features of moderately differentiated squamous cell carcinoma (Fig 3). The tumor was not involving retroperitoneal soft tissue including renal vessels, Gerota’s fascia and lymph nodes.
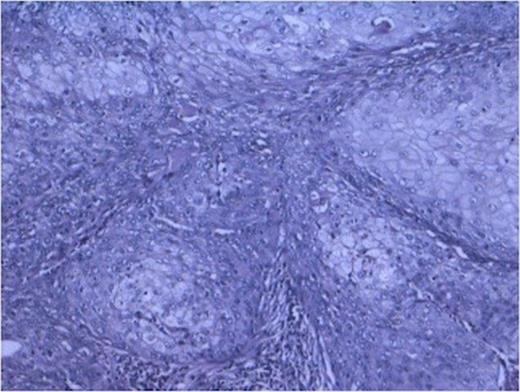
Sheets of malignant squamous cells (400x H and E stain)
DISCUSSION
Primary malignant tumors of renal pelvis are relatively rare, constituting 8-14% of all renal malignancies (4). The most common renal malignancy in adult is clear cell carcinoma followed by papillary carcinoma and chromophobe cell carcinoma (5,6). The kidney is unusual site for SCC which is known to arise from collecting system (7). Usually renal squamous cell carcinoma is highly aggressive and of a high grade at presentation.
SCC of urothelial tract is thought to arise through a process of metaplasia of urothelium. A large percentage of patients have squamous metaplasia of adjacent urothelium. Various etiological factors have been held responsible for squamous metaplasia and subsequent carcinoma. Of these renal calculi and infections are leading ones. Other factors implicated include exogenous and endogenous chemical, Vitamin A deficiency, hormonal imbalance, schistosomiasis and smoking. However, cases have been reported in which no apparent etiological factor could be detected (1,3). In our case tumor has arisen in a chronically inflamed hydronephrotic sac. Squamous metaplasia in adjacent mucosa is seen in 17-33% of patients (8). Hydronephrosis or even pylonephrosis with peritoneal abscess formation have been reported in upper urinary tract carcinoma.
Surgery is the mainstay of treatment in SCC of renal pelvis and may result in cure in patients with lower stage tumor. Systemic chemotherapy has only marginal benefit. The prognosis of SCC of renal pelvis is very poor with a median survival rate of 3.5 months. Their general poor prognosis can be attributed to a typically advanced stage at diagnosis, but stage for stage prognosis is similar for squamous and usual urothelial carcinoma.(9)
To conclude this case is reported to highlight that a diagnosis of malignancy should be considered in a long history of inflammation or infectious pathology with no known risk factors as calculi or diabetes mellitus. Careful history taking may give clue for the presence of risk factors but SCC of renal pelvis may occur in absence of any of predisposing condition. Therefore, careful and exhaustive assessment of specimen and examination of histopathological sections is mandatory to avoid any occult malignancy in such type of non-functioning kidney.

{kind=link}
{kind=link}
{kind=link}