





Abstract
We present a case of pancreatitis with secondary pseudoaneurysm formation in a branch of the hepatic artery, which fistulated into the common bile duct following endoscopic retrograde cholangiopancreatography. This aneurysm manifested itself clinically with recurrent haematemesis, and was treated by embolisation of the anterior and posterior branches of the right hepatic artery.
INTRODUCTION
Aneurysm formation after pancreatitis is well documented in the literature, caused by the digestion of arterial walls by the enzymes such as elastase released by the pancreas1. Rupture is generally considered to be a rare complication after pancreatitis, but the formation of aneurysms themselves is relatively common, occurring in 10% of patients following pancreatitis2.
Endoscopic retrograde cholangiopancreatography (ERCP) is a common procedure used both as a diagnostic and therapeutic tool in patients with biliary tree obstruction. It is considered a safe procedure and serious complications are rare; with the most common complications being pancreatits, cholangitis, bowel perforation, and bleeding from the Ampulla of Vater following sphincterotomy. However, although far rarer than any of the above the following case illustrates life-threatening and therefore significant complication following ERCP.
CASE REPORT
We present the case of a 75 year old female admitted with acute pancreatitis, deranged liver function and Gram-negative rod septicaemia. She was admitted to intensive care and magnetic resonance cholangiopancreatography carried out to determine the aetiology of the pancreatitis. This showed a 2cm filling defect in the dilated lower end of the common bile duct, suggestive of an impacted stone. Endoscopic retrograde cholangiopancreatography (ERCP) was performed 10 days later, but showed an undilated biliary system with no filling defects; despite trawling the common bile duct several times. This indicated that the stone may have been passed spontaneously.
Subsequently the patient had several episodes of haematemesis and malaena, with the patient’s haemoglobin repeatedly dropping despite transfusion. Oesophogastroduodenal (OGD) endoscopy and Computerised Tomography (CT) scan failed to identify a source. The only positive finding on CT scan was pneumobilia, most likely due to sphincterotomy during the ERCP.
The haematemesis continued and emergency laparotomy was performed. On external examination of the stomach and duodenum no obvious ulcer or induration was seen. Pyloroduodenotomy identified a small healed duodenal ulcer and fresh clots in the first part of duodenum. On palpation of the third part of duodenum, a periampullary diverticulum was identified, although it was not bleeding. The diverticulum was oversewn prior to closure. No other abnormalities were found.
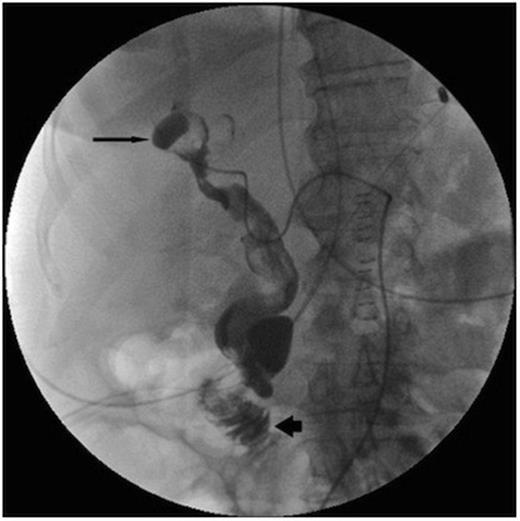
Post operatively the upper gastrointestinal bleeding continued. A second urgent OGD endoscopy showed more blood clots and fresh blood in the fundus, but once again no source for the bleeding was seen. Once the patient was stabilised an angiogram was performed. This showed a 1cm pseudoaneurysm of the right hepatic artery in the right lobe close to the Porta Hepatis. The pseudoaneurysm arose from the anterior branch of the right hepatic artery and communicated with the bile duct. The 2nd part of the duodenum was opacified, showing haemorrhage from the lesion into the duodenum via the bile duct (Figure 1).
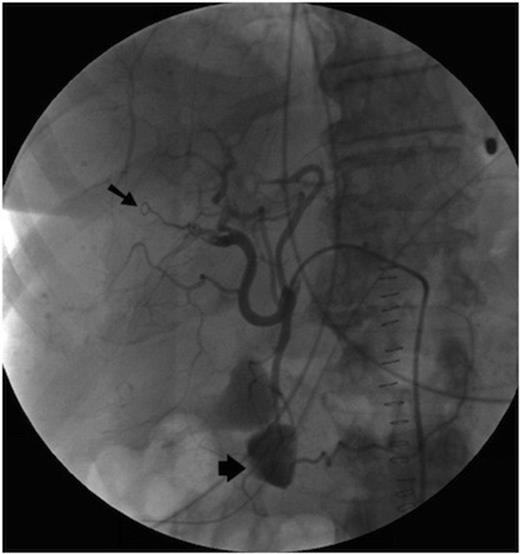
Initially, selective embolisation of the anterior right hepatic artery was performed using small coils (COOK UK) and small particles of grated gelatin sponge soaked in 0.5ml of 5% Ethanolamine. However this proved to be ineffective (Figure 2), and so the posterior branch of the right hepatic artery was embolised, successfully controlling the haemobilia. The left hepatic artery was spared.
Following the procedure there were signs of recurrent haemorrhage such as fluctuating serum haemoglobin levels and some ongoing malaena. However, these ceased spontaneously after a few days, and the patient subsequently made an uneventful recovery.
DISCUSSION
The formation of pseudoaneurysms after pancreatitis is very common, although most of these will not rupture and therefore remain asymptomatic. Cases of haematemesis following spontaneous fistulation into the biliary tree after pancreatitis are described in the literature; although often they have presented after a more severe necrotising pancreatitis3. Similar presentations have also been described with a different pancreatic source, such as a bleeding pancreatic pseudocyst4. Given that the haematemesis commenced following ERCP in this case, it is likely that it was the instrumentation of the common bile duct which led to the fisulation of the aneurysm into the biliary tree. This theory is feasible as the branches of the hepatic artery and portal vein are in very close proximity to the bile duct allowing concurrent injury to occur. We hypothesize that during the ERCP procedure the walls of the intra-hepatic bile duct and paralleling artery were injured during steel guide wire maneuvering, causing the false aneurysm. It is important to recognize that iatrogenic causes are the most common cause for haemobilia (52%)5. We also assume the bleeding in the acute recovery phase post embolisation was mainly due to the dissolving nature of the gelatin sponge. However, even though a fraction of the particles may have dissolved, the bleeding subsequently stopped as low enough perfusion pressures were maintained to stabilize the lesion.
OGD endoscopy is of course the first line investigation in any patient presenting with haematemesis, but in this case was unhelpful because there was no blood discharging from the Ampulla of Vater at the time of investigation. CT scanning lacked the sensitivity required to detect the 1cm pseudoaneurysm described in this case, though it has been successfully used in the diagnosis of larger aneurysms in other cases6. Angiography is considered the gold standard in the diagnosis of this condition7, and it is important learning point to remember this as the next line of investigation of haematemesis, particularly in patients with a history of pancreatitis. In this case there was a delay before an angiogram was done, and this delay was very nearly fatal for the patient.
Although this case report describes a rare complication of pancreatitis, it is a complication that is readily treatable provided the diagnosis is made in time. Therefore we publish it in the hope that clinicians will think of it in patients with upper gastrointestinal bleeding of unknown origin.

{kind=link}
{kind=link}