





Abstract
Sarcomatoid carcinoma is a rare tumor of the urinary bladder and accounts for approximately 0.3% of all bladder malignancies. In these tumors, histogenesis and biological behaviour remains controversial. Herein, we report a case of sarcomatoid carcinoma with osteosarcomatoid differentiation of the urinary bladder with simulataneous sigmoid colon adenocarcinoma.
INTRODUCTION
Sarcomatoid Carcinoma of the Bladder (SCB) which consists of sarcomatous and carcinomatous components simultaneously are very rare variants of Transitional Cell Carcinoma (TCC). Sarcomatoid carcinoma is known to occur in only 0.3% of total bladder cancers (1). Approximately 80 cases have been reported in the literature and most often as a single case report. In the histopathological examination of these tumors usually epithelial and connective tissue elements are seen together (2).
In this report, a case of sarcomatoid carcinoma of the bladder with osteosarcomatoid differentiation and simultaneous colonic adenocarcinoma was presented and discussed.
CASE REPORT
A 78 years old man presented with gross haematuria and serious irritative lower urinary tract symptoms. Ultrasonographic evaluation showed a mass arising from the posterior wall of bladder which completely filled the bladder lumen. Computed tomography (CT) showed a mass with hyperdense components that invaded perivesical fat about 10 cm diameter. There was no evidence of pelvic or abdominal lymphadenopathy on CT (Figure 1). Chest X-ray showed no evidence of metastasis. Eventually, we decided to perform a cystoscopy and a large, solitary, tough tumoral lesion was detected. Transurethral resection of the mass was executed and histopathological examination revealed a bladder tumor which contains both epithelial and stromal components.

CT scan showing the large heterogenous mass filling the bladder lumer
With these findings the patient underwent radical cystoprostatectomy and ileal conduit operation. Additionally, pelvic lymph node dissection was performed. During the operation, it was realised that the tumor has infiltrated sigmoid colon posteriorly and a concurrent mass of sigmoid colon was detected which has not been established radiologically in the pre-operative period. Due to these findings resection of the sigmoid colon was added to the procedure.
Histopathological examination of the specimen revealed that tumor contained high grade TCC with osteosarcomatoid differentiation. It had invaded serousal layer of the sigmoid colon and perivesical fat without lymphomatoid metastasis and without prostatic infiltration. A well differentiated adenocarcinoma with serousal layer infiltration was detected in the sigmoid colon at the same time. Microscopic findings of both tumors are shown in Figure 2.
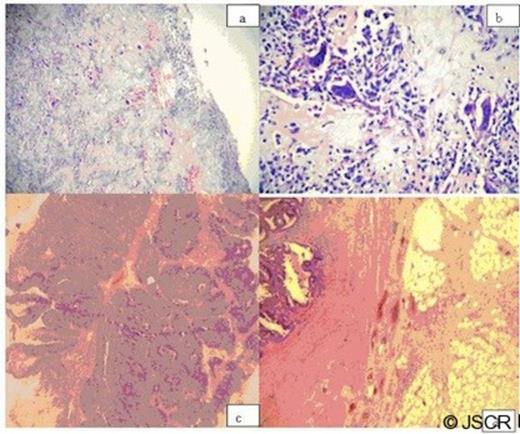
(a) The osteosarcomatous infiltration of the bladder wall charecterised by production of ostoid and osteoclastic giant cells (HE, x10). (b) View of a sarcomatous component (HE, x 60). (c) Areas of high-grade invasive urothelial carcinoma in the same case(HE, x10). (d) Sigmoid colon wall; Sarcomatous infiltration of serosal surfaces with imultaneously colonic adenocarcinoma with muscular layer infiltration (HE, x10)
After an uneventful early postoperative period, the patient and laboratory examinations were good in the follow up controls. But the patient died due to disease in the sixth month postoperatively.
DISCUSSION
The sarcomatoid carcinoma of the bladder is a very rare neoplasm with poor prognosis. The SCB consists both epithelial and mesenchymal components. The epitelial components are squamous, glandular or high grade transitional carcinoma. Whereas the mesenchymal components may be chondrosarcoma, malignant fibrous histiocytoma, osteosarcoma, leiomyosarcoma, fibrosarcoma or rhabdomyosarcoma (3). SCB is a very lethal tumor with approximately 50% mortality rate. Lopez-Beltran reported that 81% of patients with SCB (n=26) died within 9.8 months and SCB has been seen mostly in males with a mean age of 72 years. Patients usually presented with irritative lower urinary tract symptoms and gross haematuria. The great majority of the patients had advanced stage disease at the initial diagnosis (4). The overall 5-year cancer specific survival rate after cystectomy was only 20.3% (5). Because of its unfavourable histopathologic nature and rarity, there is not enough knowledge about the treatment options and prognosis of SCB in the literature. Even though transurethral resection, radical cystectomy, neoadjuvant chemoradiotherapy were the proposed treatment protocols of the SCB, radical cystectomy with adjuvant chemotherapy was the most appropriate treatment option due to the patient’s poor prognosis(6,–,9). Nevertheless mean survival rates of patients with SCB very poor and metastatic disease occurs in 66% of patients within 1 year (10).
CONCLUSION
Sarcomatoid Carcinoma of the Bladder is a very lethal and aggresive tumor with poor prognosis and more vigorous treatment protocols should be applied in such patients. Further studies with a number of cases and longer follow up periods are needed to illuminate clinical significance and prognosis of this disease, as well.

{kind=link}
{kind=link}