





Abstract
A 49 year old female presented with severe dyspnoea due to mitral regurgitation. Echocardiography revealed an aberrant mitral valve chord causing severe mitral regurgitation. The aberrant chord extended between the anterior mitral valve leaflet (AMVL) and the atrial septum causing AMVL prolapse. Resection of the aberrant chord and correction of the AMVL using synthetic Gore-Tex sutures was performed. The patient made an uneventful recovery with post-op echocardiography demonstrating normal mitral valve function.
INTRODUCTION
Functional integrity of the mitral valve and the left ventricle is crucial to maintain normal mitral valve function and adequate cardiac performance. We report about a rare congenital lesion of the subvalvular apparatus of the mitral valve which resulted in severe mitral regurgitation.
CASE REPORT
A 49 year old otherwise healthy black female presented with shortness of breath on exertion, paroxysmal nocturnal dyspnoea and orthopnoea. Her physical examination revealed a grade 4/6 pan-systolic murmur in the mitral area. Trans-thoracic and trans-esophageal echocardiogram revealed severe mitral regurgitation due to prolapse of the anterior mitral valve leaflet (AMVL), and a posteriorly directed regurgitant jet into the severely dilated left atrium was noted. An abnormal linear band was seen in the left atrium, connecting the A2 segment of the AMVL to the atrial septum and pulling the AMVL towards the left atrium (Figure 1). The left ventricle was hyperdynamic and moderately dilated. Estimated right ventricular systolic pressure was elevated to 50 mmHg, but the right ventricular function preserved. Therefore she was considered for mitral valve surgery.
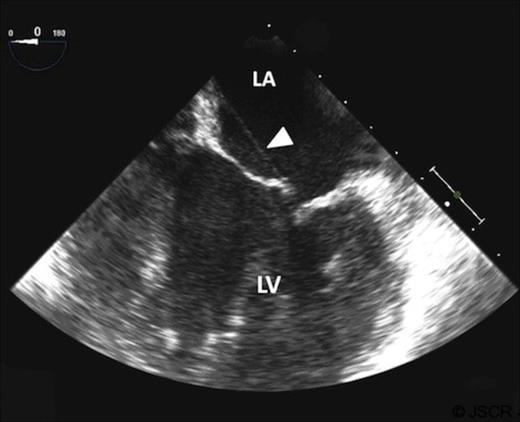
Transoesopahgeal echocardiogram showing aberrant chord in the left atrium, extending from the anterior mitral valve leaflet to the left atrial septum (white arrow).
After median sternotomy and placing the patient on cardiopulmonary bypass, the left atrium was opened through the interatrial groove. The band was identified as an aberrant mitral valve chord attached to the A2 segment of the AMVL and inserting at the fossa ovalis of the left sided atrial septum (Figure 2). In addition no appropriate chordae between the A2 segment and the papillary muscles were found. The aberrant chord was resected and two neo-chordae constructed using polytetrafluorethylene (Gore-Tex®-4, W.L. GORE & ASSOCIATES, INC) sutures. The sutures were placed into the anterior and posterior papillary muscle each and inserted into the prolapsing edge of the A2 segment. In addition, a 28 mm open Cosgrove annuloplasty band (Edwards Life sciences, Irvine, CA/US) was inserted into the posterior mitral valve ring. Tans-esophageal echocardiography after weaning off cardiopulmonary bypass demonstrated a fully functional and competent mitral valve.
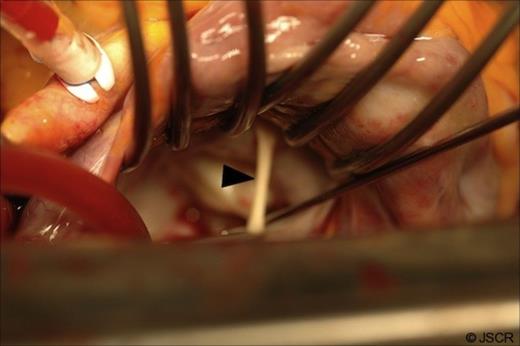
Intra operative picture after the mitral valve is exposed through the inter atrial groove, showing an aberrant chord attached to the A2 segment of the anterior mitral valve leaflet and the atrial septum (Black arrow).
The patient made an uneventful postoperative recovery and was discharged home on the fifth post operative day. Three month clinic follow up showed a marked improvement in her symptoms with normal mitral valve and left ventricular function on echocardiography.
DISCUSSION
Aberrant mitral valve chordae and in particular on the AMVL are an extremely rare finding with only a handful of cases reported in the literature [1, 2, 4]. The true chordae tendinae are fibrous strings that usually originate from the apical portion of the anterior and posterior left ventricular papillary muscles or directly from the ventricular wall, inserting into the valve leaflet. The true chordae have been termed as primary if they insert directly along the free edge of the leaflets. These chordae are primarily responsible in preventing mitral valve leaflet prolapse during systole. Secondary chordae insert in a layered fashion along the rough zone of the AMVL and are important in maintaining ventricular geometry and performance.
In our case these true chordal structures were absent in the A2 segment of the AMVL. This on its own would have resulted already in a prolapse of the A2 segment. In addition, the aberrant chord was tethering the A2 segment to the atrial septum, which severely restricted its movement and resulted in an even more severe mitral regurgitation. Given that this aberrant chord must have been present since birth it is quite surprising that it remained clinical asymptomatic until the age of 49.
Usually aberrant chordae are detected and surgically treated in patients presenting with symptoms of heart failure and severe mitral regurgitation at a much younger age [4]. A possible explanation for the delay in symptoms in our case could be that with growth and further dilatation of the left atrium, the aberrant chord pulled the AMVL more towards the atrium, resulting in an increase of leaflet prolaps and increased reversal regirgutant flow.
Surgical repair of the mitral valve always aims for restoration of normal anatomy of the whole mitral valvular complex including mitral valve leaflets, valve ring, and subvalvular apparatus. In our case the missing chordae at the A2 segment resulted in a prolapse of the AMVL. As per usual, chronic mitral regurgitation had resulted in left ventricular dilatation and enlargement of the posterior muscular portion of the mitral valve ring.
Therefore Gore-Tex® sutures, which have been shown to be ideal for chordal replacement as their strength and elasticity is similar to that of native mitral valve chordae, were used to establish normal anatomy of the AMVL. Adjustment of their length is sometimes challenging, however, in experienced hands it is a reproducible technique [4]. In addition, mitral valvuloplasty was added to stabilize the operative result. It can be performed using closed/rigid rings or open/flexible bands. In this patient with a moderately impaired ventricular function we used an open/flexible annuloplasty band, as it reduces the risk of postoperative systolic anterior movement of the AMVL and best imitates normal anatomy.
This case report not only highlights a rare cause of mitral regurgitation but also illustrates the applicability of basic principles and tools of mitral valve repair in correcting this anomaly with excellent hemodynamic results.

{kind=link}
{kind=link}