





Abstract
Entero-atmospheric fistula (EAF) is a serious complication of open abdomen (OA) treatment, especially when high output effluent leads to sepsis, electrolyte imbalance, and wound deterioration. Traditional diversion methods often cannot effectively control production. This report describes a 76-year-old man who developed a high output EAF (about 800 mL/d) after OA due to colonic necrosis and intra-abdominal sepsis. A variety of interventions (including negative pressure wound treatment adjustment, catheter bypass, and attempts to directly repair) were unsuccessful, and the fistula gradually expanded. According to the patient’s wound anatomy, a custom-made floating stoma was created using food-grade silicone, which successfully raised the fistula, shunted the effluent, and reduced chemical damage. This case shows that the low-cost and personalized silicone floating stoma can effectively control the high output EAF and protect the wound environment, which is a practical choice in the case of limited resources. Compared with many commercial isolation devices that may cost several hundred US dollars per unit, this customized silicone floating stoma can be manufactured for < $50 per patient.
Introduction
Entero-atmospheric fistula (EAF) is one of the most serious and challenging complications encountered in patients undergoing open abdominal (OA). OA refers to temporary non-closure of the abdominal wall to facilitate ongoing source control and re-exploration. EAF is a direct communication between bowel and the open wound without a mature tract, leading to uncontrolled effluent exposure. Unlike intestinal-cutaneous fistulas, EAF lacks a mature fistula structure, but directly exposes the intestinal mucosa to the external environment, resulting in uncontrollable leakage of exudate, severe fluid and electrolyte disorders, and persistent infection [1]. High-flow EAF rarely closes by itself, and effective exudate isolation is essential to protect the wound surface and allow delayed reconstruction [2]. Although a variety of isolation techniques have been described, such as improvements in negative pressure wound therapy and floating stoma devices, their effectiveness may be limited by cost, instability of equipment or difficulty in adapting to irregular wounds [3, 4].
We report a successful treatment case of a high-flow EAF using a personalized, low-cost silicone floating stoma design to improve isolation and wound stability.
Case report
A 76-year-old man presented with acute abdominal pain and bloating. Emergency examination showed intestinal necrosis, and laparotomy confirmed extensive necrosis of the ascending colon and transverse colon. Due to severe contamination and hemodynamic instability, OA was initially used to temporarily close the fascia and temporarily close the fascia. During the subsequent hospitalization in the intensive care unit, the patient developed persistent abdominal sepsis, electrolyte and acid–base balance disorders, malnutrition, and incision fat liquefaction. Despite multidisciplinary treatment, including the use of antibiotics, hemodynamic support, somatostatin infusion and total parenteral nutrition, wound conditions remained precarious.
On approximately postoperative Day 14, fecal-like effluent emerged from the abdominal wound during dressing change, revealing development of an EAF (Fig. 1A). Computed tomography confirmed that the fistula was connected to the small intestine (Fig. 1B and C). The average daily secretion was 800 ml. Attempts to control secretions, including simplified NPWT, catheter-based shunt, T-tube placement, and local repair, were unsuccessful, resulting in a gradual expansion of the fistula (Fig. 1D). Based on accurate wound measurement results, we developed a custom silicone floating stoma system. The patient’s wound contour is adapted by using a mold with an asymmetric ring structure, and then the food-grade silicone is poured into the mold to create a flexible and personalized stoma ring. The irregular substrate surface of the ring enhances the friction with the wound bed (Fig. 2A–F). After the wound was prepared, the silicone ring was placed over the fistula, fixed with a strip adhesive, and combined with the stoma bandaging system (Fig. 3A–F).
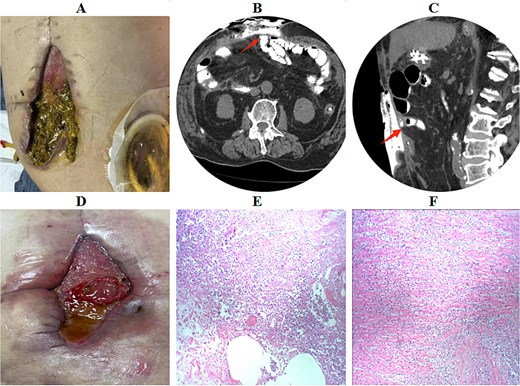
Clinical photographs and imaging findings of the EAF. (A) Appearance of the newly developed fistula in the OA. (B and C) Contrast-enhanced fistulography demonstrating communication with the small bowel. (D) Enlargement of the fistula after repeated attempts at isolation. (E and F) histopathology showing acute inflammation with focal mucosal necrosis.
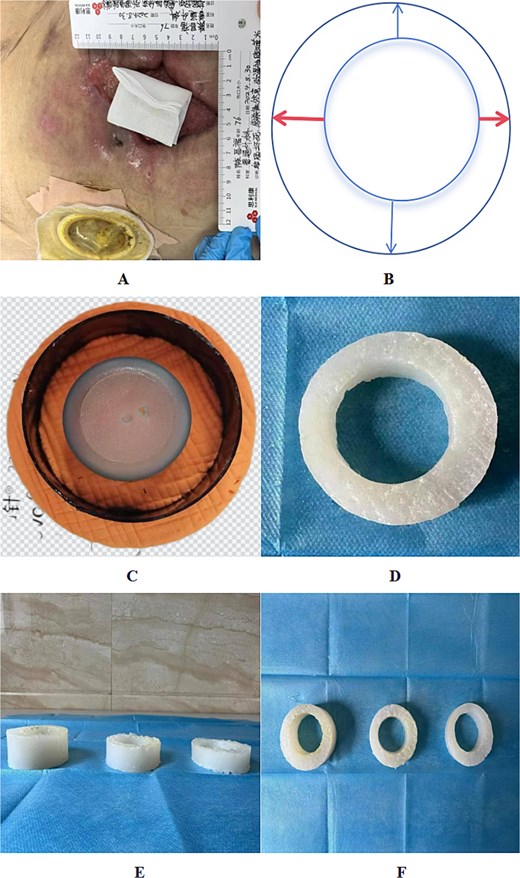
Schematic representation of customized silicone stoma fabrication process. (A) Measurement of wound dimensions and fistula-to-skin distance. (B) Determination of asymmetric ring width for improved adaptation. (C) Preparation of the lower mold base with a textured surface to enhance friction. (D) Final silicone ring following polymerization.
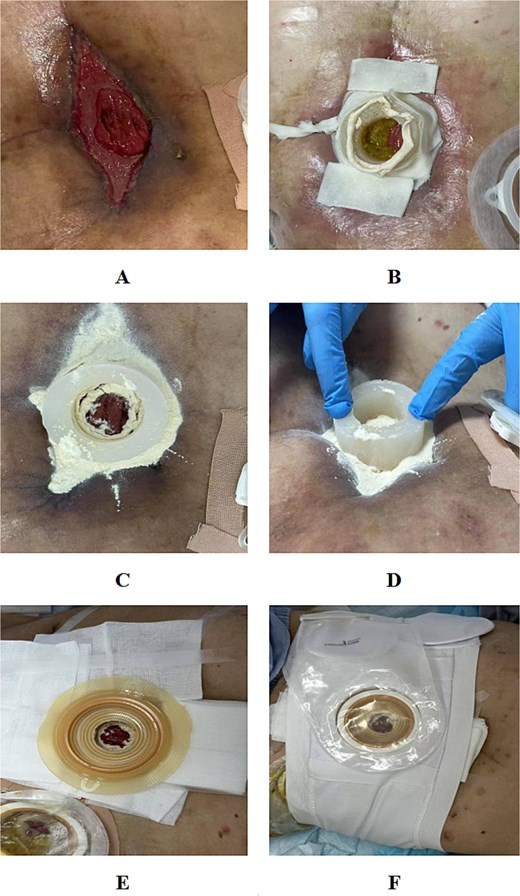
Application process of the customized silicone floating stoma. (A) Wound cleansing and preparation. (B) Shaping of the silicone ring to fit wound contours. (C) Placement of strip paste to improve adhesion. (D) Coverage of surrounding granulation tissue with petrolatum gauze. (E) Application of ostomy barrier and fixation. (F) Final configuration with ostomy pouch attached.
The device maintains a stable outflow isolation, reduces local inflammation, and improves wound condition. In the following weeks, the patient’s general condition was stable, the nutritional status was improved, and the wound environment was suitable for the final surgery. Delayed fistula resection and abdominal wall reconstruction were successfully performed through the lateral approach to minimize the damage to the adhesive intestine (Fig. 4A, C, and D). The postoperative process was smooth, and the incision healed well after 1 month of follow-up (Fig. 4B).
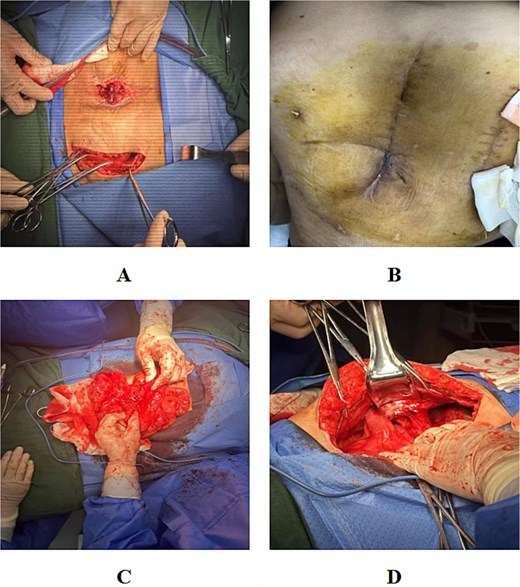
Fistulectomy and abdominal wall reconstruction. (A) Lateral surgical approach to avoid injury to exposed viscera. (B) Adhesiolysis and mobilization of the affected bowel loop. (C) Excision of the fistulous segment. (D) Well-healed postoperative incision at one-month follow-up.
Discussion
EAF is a serious complication in the treatment of intra-abdominal infections due to direct mucosal exposure, lack of protective fistula, and continuous leakage of intestinal secretions [2, 5]. These factors lead to persistent sepsis, metabolic disorders, and granulation tissue dysplasia [3].
High-flow EAF has a particularly poor prognosis and often require surgical intervention to cure [6, 7]. Traditional secretion control methods, such as modified negative pressure wound therapy, fistula intubation and shunt, are often ineffective for cases with irregular wounds, severe edema or abdominal freezing.
Floating stoma technology has attracted attention because of its ability to drain secretions from the wound surface and has become an effective shunt method [8–11]. Previous reports have described the use of prefabricated devices or 3D printed stoma components, but these methods may be costly or not available in resource-poor environments [12, 13]. In addition, firm adhesion to irregular granulation tissue is still a major technical problem.
While other techniques such as negative pressure wound therapy and catheter-based shunt methods have been widely utilized, they often face challenges in cases of irregular wounds and severe edema [1, 14, 15]. In this case, we used a custom silicone floating stoma made of readily available materials. Personalized measurement ensures a close fit with the anatomical structure of the wound. The irregular mold base provides mechanical stability, and the flexibility of the silicone allows it to adapt to changes in the contour of the wound. This method achieves stable excreta drainage, promotes the formation of granulation tissue, and can safely perform delayed surgical repair. This method is significantly more affordable compared to other commercially available stoma devices, which may cost several hundred dollars per unit. In comparison, the silicone floating stoma can be manufactured for less than $50 per patient. Food-grade silicone was selected as a pragmatic material due to its flexibility for irregular wound contours, ease of shaping, and low cost. Compared with other improvised isolation strategies and resource-intensive customized devices, this approach prioritizes rapid patient-specific fabrication using readily available materials. Limitations include the single-case design, limited follow-up, and potential device displacement; prospective series should evaluate stability and wound complications.
Because this is a single case and post-intervention serial quantitative recordings of effluent volume and wound dimensions were not captured in a standardized manner, we report qualitative clinical improvement and successful delayed reconstruction rather than time-series metrics. Future prospective series should record daily output, wound area, and device stability outcomes using predefined protocols. In addition, further studies are needed to verify its long-term effects and repeatability under different fistula morphology. However, this case shows that when conventional methods are not applicable, customized silicone stoma can be used as a practical auxiliary means for the management of complex upper gastrointestinal fistula.
Conclusion
Silicone floating stoma for patients is a simple, adaptable and low-cost technique, which can be used for the separation of high-output EAF after open abdominal surgery. This method can effectively protect the wound, improve patient stability, and support delayed definitive surgery, making it suitable for various clinical environments, especially in areas with limited resources. Although this method has shown potential application prospects, its long-term efficacy and repeatability in different fistula types still need to be fully verified by further study with larger sample size and longer follow-up period.
Author contributions
Conceptualization: Changxiao Hu, Miaoju Nie, Gang Cao.
Clinical Management: Changxiao Hu, Hong Wen.
Data Collection: Changxiao Hu, Gang Cao.
Device Development: Yuxiang Liu, Hong Wen.
Manuscript Drafting: Yuxiang Liu.
Review & Editing: Miaoju Nie, Gang Cao.
Supervision: Changxiao Hu.
Final Approval: All authors.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
No external funding was received for this study.
Ethical approval
Ethical approval was obtained from the institutional review board of Guizhou Provincial Second People’s Hospital.
Informed consent
Written informed consent for publication of this case report and accompanying images was obtained from the patient, and all potentially identifying information has been removed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}