





Abstract
Chronic anal fissures (CAF) are painful and often resistant to medical therapy. While lateral internal sphincterotomy is effective, it carries a risk of incontinence. Laser Fissuroplasty (LaFiP) is a minimally invasive alternative gaining traction globally. We report two male patients aged 28 and 47 years, respectively, with CAF unresponsive to medical therapy. Both presented with severe post-defecation anal pain and were diagnosed with posterior midline fissures. LaFiP was performed under pudendal block using 350–400 joules of energy from a 1470 nm diode laser. Postoperatively, both experienced rapid symptom resolution and complete healing within weeks, with no incontinence at 6-month follow-up. LaFiP appears to be a safe and effective technique for managing CAF, particularly suitable for patients at risk of incontinence. Although limited by a short follow-up of six months, initial results from these two cases were promising. Nonetheless, the long-term durability of the intervention requires further study.
Introduction
An anal fissure is a painful disruption in the anoderm distal to the dentate line, resulting in internal anal sphincter spasm and a reduced perfusion of the anoderm [1]. Fissures usually occur in the posterior midline and those off the midline or multiple should prompt evaluation for a specific etiology, e.g. malignancy, sexually transmitted disease, inflammatory bowel disease, tuberculosis, etc. [2].
Anal fissures can be classified as acute or chronic. Chronic anal fissures (CAF) are identified by indurated margins, absence of granulation tissue, visible internal sphincter fibers, a sentinel pile, or a fibroepithelial polyp at the apex [3]. CAFs are usually recurrent or persist beyond four weeks [4]. Anal fissures account for approximately 10% of visits to colorectal units [5] and present with severe post-defecation anal pain lasting up to two hours [6], often associated with scanty bright red bleeding per rectum.
Treatment aims to relieve pain and improve perfusion to the fissure through sphincter relaxation. While non-surgical treatment is effective for most acute fissures, the success rate is about 50%–60% for CAF [5]. Non-surgical treatments include high-fiber diets, warm sitz baths, analgesia, and chemical sphincter relaxation using botulinum toxin injections, topical nitroglycerin, or oral/topical calcium channel blockers like nifedipine or diltiazem [1, 6].
Surgical intervention is considered when conservative management fails, typically after 4–6 weeks. Surgical options include lateral internal sphincterotomy, fissurectomy, advancement flaps, and anal stretch [3]. Although lateral internal sphincterotomy has a high healing rate, it carries a considerable risk of incontinence [3]. Recently, a minimally invasive laser-based intervention, Laser Fissuroplasty (LaFiP), has gained increasing use in Europe, North Africa and Middle East [7]. The current published series on LaFiP are small and heterogeneous, hence the need for further evaluation. To the best of our knowledge, we present two cases of anal fissures among the first reported to be managed by LaFiP in sub-Saharan Africa.
Case presentation
Case 1
A 28-year-old male presented with an 18-month history of intermittent bright red bleeding per rectum during defecation, accompanied by severe anal pain graded as 9/10 on the visual analogue scale (VAS). He reported occasional constipation and pruritus ani but no tenesmus, feeling of incomplete bowel emptying or anal discharge. He had no prior medical treatment for his symptoms.
Perineal inspection revealed a posterior anal fissure and a sentinel pile (Fig. 1). However, digital rectal examination was deferred due to tenderness. There was no clinical suspicion of a specific cause of the fissure such as Crohn’s disease, tuberculosis or malignancy.

Typical finding of a CAF. CAF showing lack of granulation tissue, visible internal sphincter fibers at the base of the fissure, and a sentinel pile at the distal end of the fissure.
He underwent LaFiP under pudendal block with sedation. Using the sweeping technique, 350 joules of laser energy was applied to the fissure. The patient was pain-free following LaFiP and was discharged on postoperative day 1 on oral paracetamol for 5 days and nifedipine anal paste for one month. At two-week follow-up, his VAS pain score was 1/10 and the fissure had clinically healed. He was followed up for six months; he remained pain free, had no rectal bleeding or constipation, and a St. Mark’s incontinence score of 0/24 signifying perfect fecal continence.
Case 2
A 47-year-old man presented with a one-year history of recurrent post-defecation anal pain with a VAS score of 9/10. There was no associated bleeding per rectum or anal discharge but had pruritus ani. He had no change in bowel habits, tenesmus, feeling of incomplete bowel emptying or family history of colorectal cancer. He had previously used nifedipine anal paste for three months without symptom relief.
Examination revealed a tender posterior anal fissure. Due to pain, proctoscopy was deferred until surgery. He underwent LaFiP under pudendal block and sedation, with 400 joules of laser energy applied to the fissure to cause superficial necrosis and induce acute inflammation and healing.
He was discharged on postoperative day one on oral paracetamol for 5 days. No antibiotic prophylaxis was administered. His pain resolved within three weeks after surgery with a VAS pain score of 0/10, and by five weeks, the fissure had completely healed. At the end of six months follow-up, he remained symptom-free with preserved fecal continence and a St. Mark’s incontinence score of 0/24.
Laser Fissuroplasty technique
LaFiP was performed using a Leonardo Mini 1470 nm diode laser from Biolitec, Germany, set to continuous mode at 6 Watts (Fig. 2). The LOMA handpiece was used in a no-contact technique about 1–2 cm from the tissue to apply the laser energy onto the fissure. LaFiP began with vaporization of the papilla at the fissure apex to the level of the healthy mucosa (Fig. 3A). This was followed by continuous treatment of the ulcer in a craniocaudal direction, from right to left, using the sweeping technique. A change in tissue color from fleshy to gray was considered the endpoint of adequate treatment (Fig. 3B). The laser energy was applied for 58–60 seconds resulting in a total of 350–400 joules of energy delivered. Laser goggles were worn by the operating team as a safety precaution when the laser was in use. Postoperative management consisted of oral paracetamol, syrup lactulose, nifedipine anal paste, and sitz bath.

Leonardo mini diode laser (Biolitec Germany). Diode laser with the settings for LaFiP.
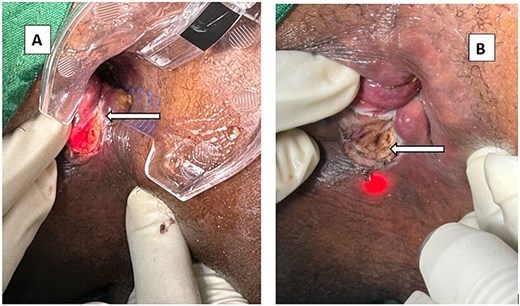
(A) The treated papilla at the apex of the fissure (arrow). Appearance of a CAF after LaFiP. (B) The tissue of the fleshy ulcer turns gray after treatment (arrow). Appearance of a CAF after LaFiP.
Discussion
Medical therapy for CAF has limited success, with about half of patients requiring surgical intervention [5], similar to our second patient who had used nifedipine anal paste for 3 months without success. Lateral internal sphincterotomy remains the gold standard, offering immediate pain relief and a healing rate of over 95% for CAF but has a 5%–15% risk of incontinence to gas or stool [1, 5].
Preliminary reports suggest that LaFiP offers satisfactory healing rates but with less risk of incontinence [6]. Laser allows for focused energy application to narrow areas, minimal tissue penetration (2–3 mm), and limited collateral spread, reducing the risk of sphincter injury. Also, LaFiP offers faster healing of fissures and return to regular activity, evident in the study by Esfahani et al. [6], which reported a return to regular activity within 1–2 days and fissure healing within 1–2 weeks after laser treatment.
The efficacy of LaFiP is secondary to the lysis of the fibrous scar overlying the ulcer of the CAF resulting in release of the tension (sphincterolysis) of the internal sphincter. This can be readily appreciated by palpating the internal sphincter before and after LaFiP. Importantly, the denatured scar is left as a protective layer over the sphincter muscle, thus preventing the exposure of the muscle to the environment.
LaFiP also stimulates an inflammatory response resulting in angiogenesis and regeneration of the submucosa and mucosa and hence converts a CAF into an acute anal fissure [6], which is amenable to conservative measures. Thus, LaFiP must be complemented with topical therapy as was done in Case 1.
There is some degree of heterogeneity among surgeons using this technique. Esfahani et al. [6] used a fractional carbon dioxide laser with a wavelength of 10 600 nm and power of 15–18 watts, while we used a Leonardo Mini 1470 nm diode laser and a power of 6 watts in our two cases. Fateh et al. [1] reported the use of diode laser for 10–20 sessions each lasting 5–10 minutes by a non-contact technique. Therefore, there is need for more research into the ideal laser wavelength and optimal energy to deliver.
This report was limited due to the short follow-up period, small sample size, and the absence of anal manometry measurements.
In conclusion, LaFiP is a safe, effective and minimally invasive technique for treating CAF. It promotes faster healing, preserves sphincter function, and avoids complications associated with traditional surgery. Its ease of use and favorable outcomes make it a promising option for wider adoption, especially in resource-limited settings like sub-Saharan Africa but will need further larger studies.
Acknowledgements
We acknowledge Biolitec Germany for providing the laser machine and probes used for the procedures.
Conflicts of interest
One co-author, Dr Peter C. Ambe is a consultant for Biolitec Germany.
Funding
No financial support was sought or received by the authors for this study.
Author contributions
All authors were involved in the management of the patients. All authors read and approved the final version of this manuscript.
Informed consent
The patients gave written informed consent to publish these case reports including clinical photographs. This was according to the local ethics requirements of the hospital.

{kind=link}
{kind=link}
{kind=link}