





Abstract
Actinomycosis is a rare chronic bacterial infection, with pelvic involvement accounting for ~5% of cases. Surgery may be required if there is intestinal obstruction, abscess formation, severe infection, or if malignancy cannot be excluded. We report a 46-year-old woman with a 12-year history of an intrauterine device, presenting with abdominal pain, vomiting, constipation, lethargy, and malaise. Examination revealed abdominal distension, tenderness, and a left iliac fossa mass. Computed tomography imaging showed a complex, infiltrative pelvic mass involving the sigmoid colon and adjacent structures, including the small bowel, causing a closed-loop small bowel obstruction and raising suspicion of malignancy. She underwent emergency laparotomy with small bowel resection and anastomosis, Hartmann’s procedure, and bilateral ureteric stent insertion. Histology confirmed actinomycosis. She recovered well and commenced a 1-year antibiotic course. Pelvic actinomycosis demands a multidisciplinary approach with combined surgical and medical management due to its complex presentation and tendency to mimic other conditions.
Introduction
Actinomycosis is an invasive, slowly progressive bacterial infection caused by the bacterium Actinomyces [1]. It results in an endogenous infection when the organism, which typically resides on mucosal surfaces, gains access to deeper tissues due to trauma, surgery, endoscopic procedures, foreign bodies, or other breaches of the mucosal barrier [2]. The incidence of actinomycosis is ~1 in 300 000, with ~20% of cases involving the abdomen [3]. Abdominal actinomycosis often presents as an inflammatory mass and can mimic conditions such as diverticulitis, inflammatory bowel disease, abscesses, and even malignancy [4]. There is overlap between clinical and radiological features, presenting significant diagnostic challenges for clinicians.
Our case report describes an unusual presentation of abdominal actinomycosis presenting as a pelvic mass with a closed-loop small bowel obstruction, necessitating urgent surgical intervention. This case underscores the importance of deceptive clinical and radiological presentation in abdominal actinomycosis and the role of surgery in its management.
Case report
A 46-year-old woman, previously healthy and fit, presented to the accident and emergency department with a 3-month history of worsening abdominal pain and vomiting, accompanied by lethargy and malaise. She also reported alternating diarrhoea and constipation over the past few weeks. She had an intrauterine contraceptive device (IUD) for 12 years. There was no significant past medical or surgical history. The surgical team examined her. Her observations were stable, and on clinical examination, she had a distended abdomen with tenderness in the lower abdomen and a lump in the left iliac fossa. Her blood tests are listed in Table 1.
Blood investigations
| Investigation | Results |
|---|---|
| Hemoglobin | 90 g/L |
| White blood cells | 9.6 × 109/L |
| Serum C-reactive protein | 143 mg/L |
| Serum CA 125 | 37 U/mL |
| Serum carcinoembryonic antigen | 1.4 ng/mL |
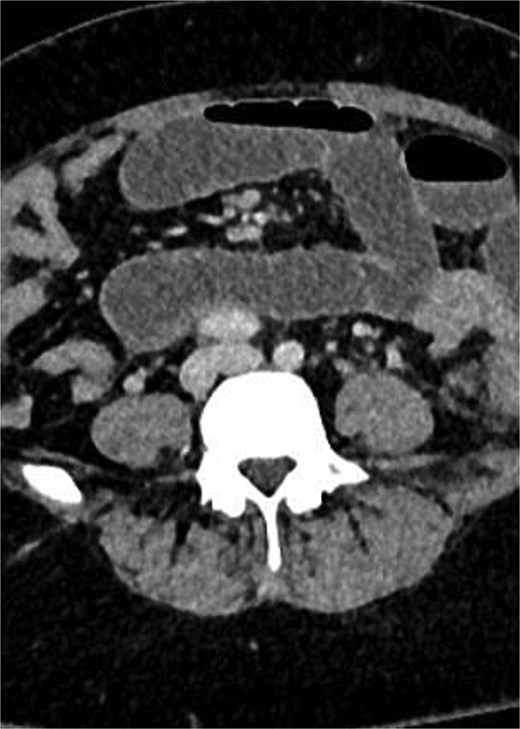
A computed tomography (CT) scan of the abdomen and pelvis showed complex and aggressive disease involving the pelvic area, affecting the urinary bladder, cervix, sigmoid colon, and the left adnexa. Additionally, a loop of small bowel was involved in the inflammatory process, leading to a closed-loop small bowel obstruction. Differential diagnoses included infiltrative malignancy, tuberculosis, or actinomycosis. A CT scan of the thorax was performed to rule out any pathology or metastasis to the lungs.
CT images with Fig. 1: Pelvic mass involving sigmoid colon, uterus, urinary bladder, left fallopian tube and ovary. Figure 2: Small bowel obstruction secondary to the mass.

CT scan of abdomen and pelvis: Pelvic mass involving sigmoid colon, uterus, urinary bladder, left fallopian tube and ovary.
CT scan of abdomen and pelvis: Obstructed loop of small bowel.
The patient underwent an emergency exploratory laparotomy. Intraoperative findings revealed a large, inflammatory mass involving the sigmoid colon, a loop of small bowel, the left fallopian tube and ovaries, the uterus, and the urinary bladder. The adherent small bowel was resected en bloc with the sigmoid mass. We divided the proximal and distal loops of small bowel and performed an isoperistaltic side-to-side stapled anastomosis using a linear cutting stapler. The left ureter could not be identified separately from the mass; therefore, the on-call urologist was consulted. The urologist performed a cystoscopy and bilateral ureteric stent insertions, along with a bladder biopsy. A sigmoid colectomy was carried out, mobilizing the colon while preserving the left ureter. A gynaecological oncologist joined the operation to assess the uterus and adnexa and assist in separating the mass from the bladder and adnexa. An end colostomy was performed, and the abdomen was closed. Histology of the sigmoid colon and small bowel showed an inflammatory mass with morphological features suggestive of Actinomyces. The bladder biopsy exhibited reactive changes. Her IUD was removed post-operatively by the gynaecology team due to intermittent vaginal bleeding. She was followed up by the general surgeons in the outpatient clinic and was doing well. She was also monitored by urology and had her ureteric stents removed.
Discussion
Actinomyces spp. are Gram-positive bacilli that form part of the commensal flora of the oropharynx, gastrointestinal, and genitourinary systems in humans [5]. Humans serve as the natural reservoir for this bacterium, with four types of infection identified: cervicofacial, thoracic, abdominopelvic, and cerebral [6]. Actinomycosis is a granulomatous inflammation that may present as a sinus, fistula, abscess, or inflammatory pseudotumour [7]. Pelvic actinomycosis can occur at any age and typically presents with a mass involving the urinary bladder, rectum, sigmoid colon, and other pelvic organs [8]. Patients may also present with frozen pelvis and a solid, fixed mass with indistinct boundaries, sometimes accompanied by secondary hydronephrosis [9]. IUDs increase the risk of actinomycosis by damaging the normal uterine mucosa and may present with disease mimicking abdominal malignancy, which explains the disease in our patient [10]. Diagnosis is difficult pre-operatively, as it can be challenging to differentiate from malignancy, tuberculosis, and endometriosis. This explains why many patients, including ours, present with findings suspicious of malignancy [11]. Patients present with abdominal pain, weight loss, anorexia, and vaginal discharge. CA125 can be mildly elevated in pelvic actinomycosis, as demonstrated in our case [12]. Diagnosis of pelvic actinomycosis is often confirmed on histology postoperatively. Histology shows yellow sulphur granules, chronic granulomas with fibrous stromas, and cyst-like spaces [13]. Actinomycosis infection is usually treated with antibiotics, but a pelvic mass warrants surgical intervention, especially when it presents with bowel obstruction, fistula, abscess, or when malignancy cannot be excluded. Surgery is tailored according to the pathological presentation. Our patient presented with a closed-loop small bowel obstruction with a sigmoid mass, both necessitating surgical intervention. The small bowel loop adherent to the sigmoid mass needed excision, with primary anastomosis of the afferent and efferent loops. Prolonged antibiotic therapy is recommended, with penicillin G and amoxicillin commonly prescribed for the condition [14].
Conclusion
Pelvic actinomycosis can mimic various intra-abdominal pathologies and often raises concern for malignancy due to its infiltrative nature. Acute presentations, such as intestinal obstruction—particularly closed-loop small bowel obstruction—require early surgical intervention. Optimal management involves a multidisciplinary approach that includes appropriate surgical treatment, input from infectious diseases and microbiology specialists, and prolonged antibiotic therapy.
Conflicts of interest
No conflicts of interest.
Funding
None declared.

{kind=link}
{kind=link}