





Abstract
Internal hernias secondary to congenital mesenteric defects are a rare cause of small bowel obstruction (SBO) in adults. Additionally, the identification of chronic congenital mesenteric defects and congenital bands is notably rare. Herein, we report the case of an 18-year-old man presenting with acute abdominal pain and bilious vomiting, without constipation or distention. Contrast enhanced computed tomography demonstrated dilated small bowel loops consistent with obstruction. Emergency laparoscopy revealed internal herniation of the small bowel through a congenital mesenteric defect, along with two fibrous congenital bands. The procedure was converted to laparotomy, during which the bands were divided, the hernia was reduced, and the mesenteric defect was closed. The patient recovered uneventfully. This case highlights the diagnostic challenges of congenital internal hernias causing SBO in adults and reinforces the importance of maintaining awareness of this rare entity in the evaluation of SBO in the virgin abdomen.
Introduction
Internal hernias are an uncommon cause of small bowel obstruction (SBO), accounting for <6% of cases [1]. They are defined as the protrusion of a viscus through a peritoneal or mesenteric defect, which may be congenital or acquired. Congenital internal hernias typically arise from abnormal embryological development of the mesentery, leaving defects or abnormal peritoneal folds through which bowel may herniate [2]. While these anomalies are most frequently recognized in neonates and children, their presentation in adulthood is rare and often diagnostically challenging. Additionally, internal hernia can result in incomplete bowel obstruction, producing symptoms which can mimic other causes of the acute abdomen which can delay diagnosis. We report the case of an adult patient who developed SBO secondary to chronic internal herniation through a congenital mesenteric defect, with associated congenital bands, without congenital malrotation. This case illustrates the diagnostic challenge inherent to such rare anomalies and highlights the importance of early surgical intervention to prevent bowel ischaemia and the need for resection.
Case report
Presentation
An 18-year-old man presented to the emergency department (ED) with a 1-day history of worsening diffuse abdominal pain. He also reported copious bilious, non-bloody, non-faeculent vomiting. He reported opening his bowels the morning of the presentation and reported passing flatus while in the ED. He denied abdominal distention or fevers. Historically, the patient reported three other episodes of upper abdominal pain, which were less severe and self-limiting. These episodes had recurred most recently one week prior to his presentation. He has no past medical history, took no regular medication, and has no known drug allergies. His surgical history included tonsillectomy in childhood. He is a never-smoker, drinks less than three units of alcohol weekly, and has no history of recreational drug use. He has no relevant family history.
Examination and initial investigations
On admission, he was stable. Examination demonstrated normal vital signs, diffuse abdominal tenderness with guarding in the epigastrium. The abdomen was not distended. There were no palpable masses and no peritonitis. Biochemical and haematological parameters revealed a lactate of 2.4 mmol/L and white cell count of 21.6 × 109/L and were otherwise unremarkable. Intravenous (IV) contrast-enhanced computed tomography (CT) of the abdomen and pelvis revealed distended stomach and dilated loops of small bowel with inflammatory change in the mesentery, and an apparent twist in the root of the small bowel mesentery (Fig. 1). A diagnosis of SBO of uncertain aetiology was made.

CT image.
Management
The patient received fluid resuscitation and was kept nil by mouth. Emergency diagnostic laparoscopy demonstrated internal herniation of the small bowel though a congenital mesenteric defect near the duodenal-jejunal flexure. The mesentery though which the bowel was herniated demonstrated significant fibrous change, consistent with a chronic defect. The herniated bowel was healthy, with active peristalsis and no ischaemia or perforation. No congenital malrotation was identified. Additionally, two fibrous congenital bands were identified. One band extended from the mesentery of the transverse colon to the distal small bowel, with the subsequent fibrous band extending from the proximal to distal small bowel mesentery (Fig. 2). Focal narrowing of loops of small bowel which were interposed between the congenital bands was identified. It was not possible to safely reduce the internal hernia laparoscopically and on this basis the operation was converted to open laparotomy (Fig. 3). The patient underwent reduction of the internal hernia, and the mesenteric defect was repaired with 3–0 vicryl™ (polyglactin 910, Ethicon, Somerville, NJ, USA). No bowel resection was required. Adhesiolysis of the fibrous congenital bands was also performed.

Laparoscopy images.
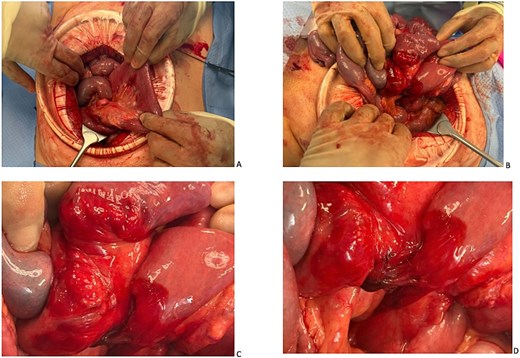
Laparotomy images.
Outcome
The patient’s post-operative course was standard and without complication, he progressed to complete normal diet by Day 3 post-operative with bowels opening on Day 5 post-operative. Histology from the fibrous congenital bands demonstrated ‘one fragment of fibroconnective tissue focally showing a foreign body type giant cell recreation to polarizable material and a second fragment of tissue showing marked haemorrhage, vascular congestion and oedema’. He was discharged well on post-operative Day 5, and remains well, with ongoing follow up.
Discussion
Internal hernias are an uncommon cause of SBO accounting for ~6% of cases [1], with congenital internal hernias being particularly rare [2]. While these anomalies are recognized in childhood, their presentation in adulthood is rare and often diagnostically challenging. Several subtypes of congenital internal hernia have been defined based on location with transmesenteric, as in this case, representing just 8% [3]. Congenital internal hernia may present non-specifically, either insidiously with recurrent episodes of abdominal pain or with features of acute obstruction, with both seen in this case. Where they present emergently, symptoms may include generalized abdominal pain, distension, bilious vomiting, and constipation. In adults, the absence of prior abdominal surgery —the so-called ‘virgin abdomen’—may reduce suspicion for obstruction in favour of other differential diagnoses. In certain cases, such as this, on thorough history taking there may be reports of previous episodes of self-resolving abdominal pain, which may raise suspicion.
A review of the literature demonstrates that adult presentations of congenital mesenteric defects and associated bands remain rare, with most of the available evidence limited to case reports and small series. The published literature consistently highlights the diagnostic challenge in adults, as mesenteric defects are more commonly recognized in paediatric populations and may present atypically when encountered later in life [1, 2, 4, 5]. Imaging with IV contrast enhanced CT can demonstrate suggestive features such as clustered small bowel loops, displacement of mesenteric vessels, or a mesenteric ‘whirl sign,’ but in many cases—including our own—definitive diagnosis is achieved intraoperatively [6]. However, the subtlety of radiological features means that missed diagnoses are common, particularly when there is no high index of clinical suspicion. Indeed, in several published case reports, diagnosis was only confirmed intraoperatively, as in our case [4, 7]. Surgical management across reported cases has focused on reduction of the hernia, resection of non-viable bowel when necessary, and closure of the mesenteric aperture to prevent recurrence [7]. In our patient, timely laparotomy facilitated successful reduction of the herniated loops and closure of the mesenteric defect without the need for resection, thereby averting significant morbidity. Outcomes are favourable when prompt intervention is undertaken, but delays can result in volvulus, ischaemia, or extensive resection [4, 7]. Unlike most published adult cases, which report malrotation or a single mesenteric aperture, our patient had both a mesenteric defect and multiple congenital fibrous bands, making this presentation particularly uncommon. Given the paucity of higher-level evidence, the reporting of individual cases remains important. These reports collectively underscore the variability in presentation and the importance of early recognition.
In conclusion, internal herniation through a congenital mesenteric defect associated with fibrous congenital bands is a rare cause of acute SBO in adults. This case highlights important clinical lessons. Firstly, SBO should be considered even in adults who present with non-specific features. Secondly, congenital anomalies should not be excluded in adults presenting with SBO. Thirdly, while imaging may be valuable, diagnostic laparoscopy should not be delayed where there is clinical concern for obstruction. Reporting such cases adds to the limited body of literature and may assist in guiding future recognition and management of this rare condition.
Author contributions
Níamh M. Smyth and Muhammad Zeshan contributed equally to this paper. Níamh M. Smyth (Drafting, Editing), Muhammad Zeshan (Drafting, Editing), Vikram Tewatia (Editing), Himanshu Yadav (Editing), Jim Byrne (Editing), Kaotharat Balogun (Editing), David Kearney (Clinical expertise, Editing). All authors approved final submission of the manuscript.
Conflicts of interest
None declared.
Funding
None declared.
Consent
Patient consent for publication of the case and clinical photographs was obtained.

{kind=link}
{kind=link}
{kind=link}