





Abstract
Rectal stenosis (RS) is a rare variant of anorectal malformation, characterized by a normally positioned anus with well-developed functional sphincters. An inaccurate diagnosis of RS may affect the choice of surgical procedure. We present a case of RS diagnosed via anoscopy and treated with transanal surgery. A 2-day-old male infant presented with failure to pass meconium and abdominal distension. Although the anus was normally positioned, catheter insertion was obstructed at slightly more than 1 cm. Anoscopy revealed a rectal web with an orifice, enabling catheter decompression. Web resection and strictureplasty were performed on Day 5. The postoperative course was favorable, and bougie dilation was discontinued 1 year postoperatively. Anoscopy is easily performed at the initial visit and facilitates the detection of a web with an orifice, even when it is barely visible externally. This approach enables safe catheter insertion and appropriate surgical planning.
Introduction
Anorectal malformations (ARM) occur in approximately 1 per 5000 live births annually, and rectal atresia (RA), and rectal stenosis (RS) are rare variants of ARM, with an incidence of 1% among all ARMs [1]. Sharma and Gupta classified RA into five types, with Type I defined as RS presenting as intramural stenosis or a web with a hole [2]. Patients with RA or RS require surgical intervention owing to the clinical impacts of these diseases, such as failure to pass meconium, bowel distension or perforation, and eventual sepsis. In this report, we present a case of congenital RS diagnosed using an anoscope and treated with transanal surgery.
Case presentation
A 2-day-old male infant (birth weight 2618 g) was transferred to our department due to failure to pass meconium, vomiting, and abdominal distension. He was born spontaneously late pre-term after an uncomplicated delivery. Physical examination revealed abdominal distension and a normally positioned anus (Fig. 1). Abdominal X-ray revealed diffuse bowel distension, especially a dilated sigmoid colon (Fig. 2). We attempted suction of the meconium using a silicon catheter; however, the catheter could not be advanced >1 cm through the anal orifice. We subsequently tried to evaluate the rectoanal region using an anoscope and identified a rectal web with an orifice approximately 1 cm from the anal verge (Fig. 3a). We dilated the orifice using catheters measuring 4–10 Fr and placed the catheter beyond the orifice (Fig. 3b). Subsequently, meconium passage was confirmed. Abdominal ultrasonography confirmed the catheter positioned within the rectum (Fig. 4) and also revealed that no presacral mass existed. Lower gastrointestinal fluoroscopy showed the web located approximately 1 cm from the anal verge, with no fistula between the rectum and urethra (Fig. 5a). The images also showed contrast medium stopping above the pubococcygeal (PC) line (Fig. 5b). Following transanal decompression, definitive surgery was performed on Day 5 of life. Intraoperative findings showed that the stricture was located slightly more than 1 cm from the dentate line, and it consisted of a web with a hole (Fig. 6). RS was diagnosed based on these findings, and resection of the web and strictureplasty were performed. Although bougie dilation was required postoperatively, it was gradually tapered and discontinued by 1 year after surgery. No signs of restenosis were noted. Although bougie dilation was required postoperatively, the frequency of dilation decreased gradually and was no longer necessary 1 year after surgery.

Physical examination of the patient’s anus. Initial physical examination revealed that the anus was in the normal position (arrow).
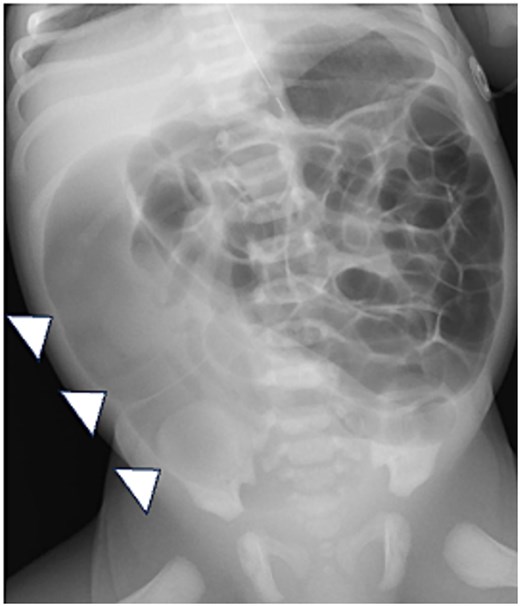
Abdominal X-ray. The X-ray shows diffuse intestinal and colonic distension, especially a dilated sigmoid colon (arrowheads).
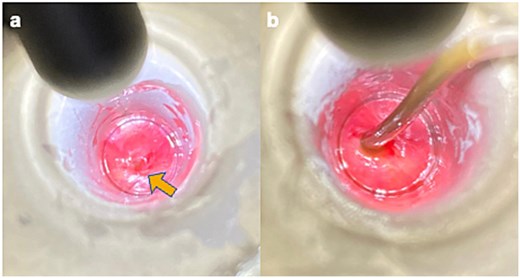
Initial anoscopy examination findings. (a) A rectal web with an orifice (arrow) is observed approximately 1 cm from the anal verge. (b) Dilation of the orifice was performed using catheters ranging in size from 4 Fr to 10Fr, and the 10-Fr catheter was placed through and beyond the orifice.
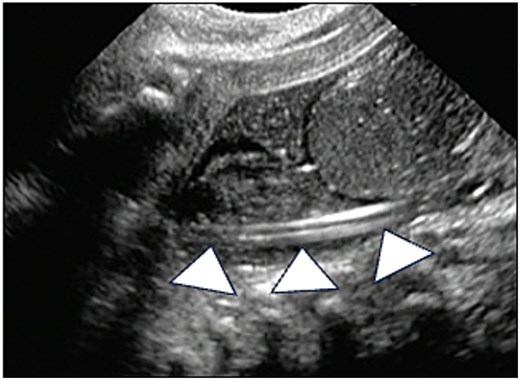
Abdominal ultrasonography. Abdominal ultrasonography showing that the catheter is positioned within the rectum (arrowheads).
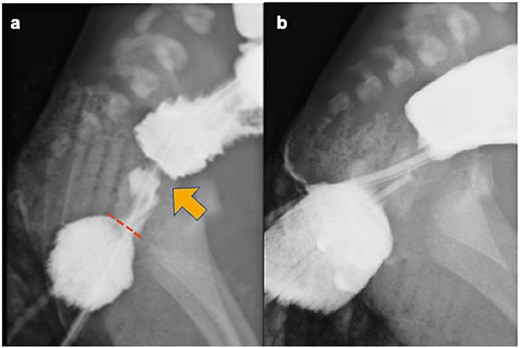
Contrast enema. (a) Preoperative contrast enema showing the rectal web (arrow) located approximately 1 cm from the anal verge (dotted line), with no fistula between the rectum and urethra. (b) Preoperative contrast enema revealing contrast medium stopping above the PC line.
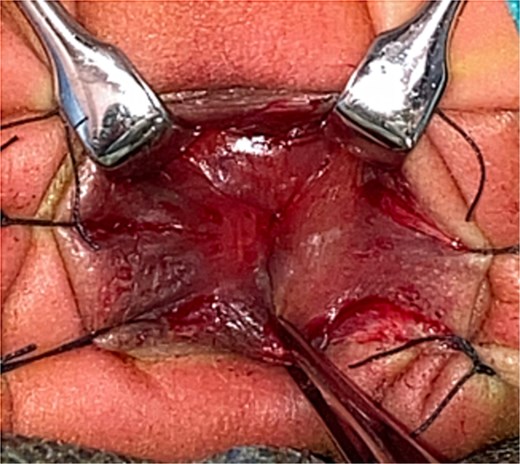
Intraoperative image. Intraoperative findings showing that the lower portion is an anal canal in the normal location, and the stricture, which consisted of a membrane with an orifice, was at a depth of approximately 1 cm. The position of the anal verge was at normal depth.
Discussion
To our knowledge, this is the first report describing direct visualization of a rectal web with an orifice via anoscopy in a patient with RS. This approach enabled rectal decompression and definitive surgical treatment.
While cardiac and skeletal anomalies have been reported in approximately 30% of cases, RA and RS generally have no associated fistula with the urogenital system [3, 4]. Due to the rarity of RA and RS, reports on long-term outcomes are limited, but functional outcomes are generally considered favorable. Although de Beaufort et al. [4] reported that over half of the patients experienced constipation and one-third required bowel management (laxatives or enemas), few patients’ experienced social difficulties during the 5-year follow-up.
Patients with RA and RS present with progressive abdominal distension, vomiting, and failure to pass meconium despite a normal anal opening on neonatal inspection. RS may manifest as delayed passage, mimicking Hirschsprung’s disease. Diagnosis can be supported by bedside catheter insertion [5], contrast enema [6], and endoscopy [7]. However, differentiating RS from RA is difficult if the opening is minute, potentially leading to unnecessary colostomy [2]. Anoscopy facilitates differentiation of these diseases by enabling direct visualization of the membranous web and accurate identification of the orifice. In our case, RS was diagnosed via direct visualization of the stricture using an anoscope. Since the presence of a normal anus does not exclude RS or RA, rectal catheter insertion is generally considered a useful diagnostic tool. However, blind insertion carries the risk of rectal mucosal injury or even perforation. In contrast, anoscopy is easily performed at the initial visit, facilitating safe placement of a decompression tube and enabling elective surgery after adequate evaluation.
Various surgical approaches to treat RA and RS have been described, such as posterior sagittal anorectoplasty (PSARP) [8], pull-through procedure [9], transanal recto-anal anastomosis [10], and transanal mucosectomy. While PSARP is commonly performed, the transanal procedure preserves local pelvic anatomy with minimal tissue damage [10]. A diversion colostomy may be required if a diagnosis of RA or RS cannot be established. Therefore, it is crucial to establish a diagnosis at the initial consultation. Rectal dilation might be a valid primary option without surgery, as reports indicate no significant difference in bowel management outcomes compared with surgery [11]. The dilation is also effective with web-type RS, but most reported cases have undergone web resection owing to concerns about restenosis [5]. Severe or fibrotic stenosis may be less responsive to dilation [11]. Additionally, a presacral mass must be carefully ruled out before dilation to prevent treatment failure. Screening for associated anomalies is also essential, as RS may coexist with Currarino syndrome and cloacal malformations [12, 13]. In our case, no associated malformations were observed. For this patient with Type I RA presenting as a web with an orifice, we performed transanal excision of the mucosal web. This decision was based on the distal location of the stricture, which allowed for a transanal approach, and the risk of restenosis associated with the extremely narrow orifice if managed by dilation alone. Although temporary dilation was required in the early postoperative period, no further dilation is currently necessary, and the functional outcome is favorable.
Conclusion
In conclusion, we described a case of RS diagnosed via anoscopy, which revealed a mucosal web with an orifice. Anoscopy is easily performed at the initial visit and facilitates the detection of a web with a hole, even when it is barely visible on external inspection. This approach enables safe catheter insertion and appropriate surgical planning, allowing for the avoidance of unnecessary stoma creation.
Acknowledgements
We thank Jane Charbonneau, DVM, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Author contributions
K.H. and Y.K. performed the catheter insertion. K.H. and Y.K. were major contributors to the writing of the manuscript. Y.K., Y.S., S.Y., Y.N., T.S., T.K., K.M., Y.O., and Y.T. contributed to the critical revision of the manuscript. All authors read and approved the final manuscript.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
None declared.
Data availability
The patient’s data are unavailable because of the need to protect personal information.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Written informed consent for publication was obtained from the parents of the patient described in this article.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}