





Abstract
We present a case of a 51-year-old male with a colonic adenocarcinoma that presented as a full-thickness rectal prolapse with external haemorrhoids. This patient had no significant medical or surgical history and presented to the emergency department with a rectal prolapse which had become incarcerated and increasingly painful over the previous 2 weeks. A computed tomography (CT) abdomen and pelvis appeared benign, demonstrating a full-thickness rectal prolapse with no definite rectal mass. A colonoscopy was performed, revealing anterior rectal mucosal edema, fibrosis, and a possible mass. This prompted the patient to be taken to the operating room for a low anterior resection of the rectum and sigmoid. A 10.5 × 8.2 × 1.9 cm rectal mass was noted and pathology revealed colonic adenocarcinoma. This case highlights the importance of performing a colonoscopy in patients with atypical rectal prolapse, even when the physical exam and CT appears benign.
Introduction
Rectal prolapse is a rare condition, affecting ~0.5% of the population, and is most often seen in elderly females [1]. When it occurs in men, they are typically under 40 years old. A growing number of rectal or sigmoid carcinoma presenting as rectal prolapse have been reported, with most noting an unusual mass or appearance to the prolapse [2–13]. We present a unique case of a 51-year-old male with an incarcerated rectal prolapse who was diagnosed with colonic adenocarcinoma despite a benign appearing physical exam and computed tomography (CT).
Case report
A 51-year-old male with no significant medical or surgical history presented to the emergency department with rectal pain, prolapse, and bleeding. The patient reported prolapsing after bowel movements for the last several months, which he was originally able to self-reduce. For the last two weeks, it had become intermittently painful and non-reducible leading him to present to the ED. He reported an intermittent history of constipation but denies history of excessive straining, with his last bowel movement being earlier that day. The patient acknowledged an unintentional 20-pound weight loss over the last several months. He reported a history of difficulty voiding associated with the prolapse. Patient denied any abdominal pain, nausea, vomiting, fevers, or chills and denied prior colonoscopy.
On arrival his haemoglobin was 10.2 g/dl (reference range 12.8–16.3 g/dl) and white blood cell count was 8.1 B/L (reference range 3.7–10.5 B/L) with neutrophilia (79.9%, reference range 40%–73%). On exam, the prolapse appeared to be full thickness with external hemorrhoids (Fig. 1). It was unable to be reduced at bedside therefore sugar was placed on the mucosa. A CT of the abdomen and pelvis with IV contrast was ordered and demonstrated a large rectal prolapse with extensive haemorrhoids and perirectal edema (Fig. 2). No definite rectal mass was noted. There was mild wall thickening of the sigmoid colon and constipation changes in the ascending and transverse colon. The following day the prolapse was temporarily reduced and the patient underwent a colonoscopy, demonstrating anterior rectal mucosal edema, fibrosis, and a possible mass. There was a rectosigmoid stricture 25 cm from the anal verge revealing friable edematous mucosa in the anterior rectal quadrant. Biopsies were taken and the decision was made to proceed with a proctectomy with end-colostomy. This procedure was performed prior to the return of biopsy results due to patient preference and our high index of suspicion for neoplasia.

Rectal prolapse. Photograph showing prolapsed rectum and external hemorrhoids observed during physician exam on admission.

CT scan of the rectal prolapse. CT of abdomen and pelvis revealed a large rectal prolapse with extensive hemorrhoids and perirectal edema.
Written consent was obtained for a robotic assisted diagnostic laparoscopic procedure and low anterior resection (LAR) of the rectum and sigmoid colon. An abdominoperineal resection was considered but avoided due to wound healing risks. In the operating room the patient’s sigmoid colon was noted to be extensively dilated (lumen measuring up to 7.7 cm in diameter) and redundant (21 cm in length was removed). The rectum was noted to have a friable papillary polypoid solid mass, measuring 10.5 × 8.2 × 1.9 cm obstructing 10% of the rectal lumen.
On postoperative day 3 the patient began to have ostomy function. The patient was discharged on postoperative day 5 with a JP drain in place which was removed 2 weeks later at his outpatient follow up appointment.
Histopathology report of the resected rectum confirmed moderately differentiated invasive colonic adenocarcinoma 1.5 cm pT2N0 (0/18 lymph nodes) (Fig. 3). The distal margin was focally positive for low-grade dysplasia. Pathology results were reviewed with the patient at outpatient follow up. An intersphincteric proctectomy with levatorplasty was scheduled and a carcinoembryonic antigen (CEA) and CT chest was ordered. CEA was elevated at 13.4 one month following his LAR. CT chest showed a suspicious lung mass, prompting a positron emission tomography (PET) scan. Although the lung mass was no longer present on the PET scan, it did demonstrate metastasis to the right hepatic lobe, for which a wedge resection was performed.
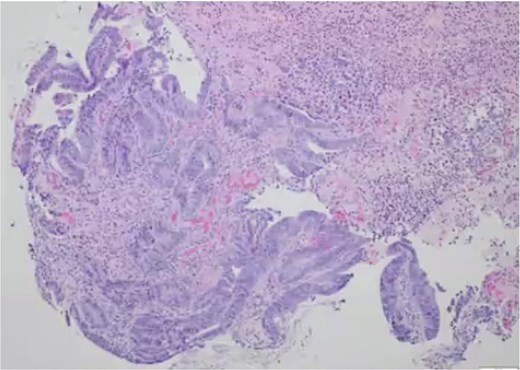
Pathology slide of rectal biopsy. Pathology of rectal biopsy demonstrating tubulovillous adenoma with focal high-grade dysplasia.
Discussion
Malignancy presenting as prolapse is uncommon but documented [2–14]. There has been debate regarding whether rectal carcinoma is a lead point causing prolapse, similar to the mechanism in intussusception, or whether chronic straining and irritation of mucosa leads to the development of colorectal cancer [3]. Our patient reported only an intermittent history of constipation, denied prolonged history of excessive straining, and had an acute prolapse, supporting carcinoma as the lead point. Lesions obstruct the canal, causing patients to strain to have bowel movement. Up to 93% of adult intussusception cases are due to malignancy [15]. When intussusception causes prolapse, the rectum may be edematous, ulcerated, folded, and non-distended, which can mask mucosal lesions on CT [16].
In our case, physical exam and CT scan demonstrated what was thought to be a full-thickness rectal prolapse in conjunction with external hemorrhoids. It was not until the colonoscopy when an unusual mass was visualized. The American Society of Colon and Rectal Surgeons provide a strong recommendation based on moderate-quality evidence, 1B suggesting the selective use of additional testing to refine the diagnosis and identify coexisting pathology [17]. This case underscores that rectal prolapse in atypical demographics (middle-aged male, short duration, weight loss) should prompt thorough malignancy evaluation, including a mandatory colonoscopy, regardless of CT or exam findings.
This patient’s pathology revealed a tubulovillous adenoma with focal high-grade dysplasia and adjacent ulceration, ultimately classified as a moderately differentiated invasive colonic adenocarcinoma with invasion into the muscularis propria (Fig. 3). About 18 regional lymph nodes were examined, all of which were negative for metastatic disease (pN0), exceeding the recommended minimum of 12 nodes for accurate pathologic staging. Although T2N0 colorectal tumors generally carry an excellent prognosis, a subset of biologically aggressive cancers has been shown to undergo early hematogenous dissemination with relative bypass of the lymphatic system [18, 19]. The presence of distant metastases in this patient despite adequate lymph node sampling and negative nodal involvement suggests either high-risk pathologic features or an intrinsically aggressive tumour phenotype with a preferential hematogenous spread. Performing a colonoscopy on this patient despite negative imaging findings on this patient was critical.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}