





Abstract
The effectiveness and safety of cryoablation for lung cancer treatment has been gaining interest. This report presents a case of robotic portal right upper lobectomy for a second recurrence post-cryoablation, with valuable pathological findings. A 58-year-old male patient was referred to our hospital for lung cancer recurrence post-cryoablation, and he underwent robotic portal right upper lobectomy and mediastinal lymph node dissection. Microscopically, papillary adenocarcinoma, fibrosis, and a foreign body reaction were observed. The patient was diagnosed with local recurrence of adenocarcinoma following cryoablation.
Introduction
Cryoablation is a treatment for malignant tumors that originated in the mid-19th century by James Arnott [1]. It triggers apoptosis and necrosis in tumor cells by freezing them using a cryoprobe and nitrogen. Interest in cryoablation as an alternative to surgical resection has grown recently; however, evidence regarding cryoablation effectiveness as a cancer treatment is limited [2, 3]. This report presents a case of second recurrence following cryoablation that was treated with robotic portal lobectomy.
Case presentation
A 58-year-old male smoker with a 9-pack-year history was referred to our hospital due to suspicion of a second lung cancer recurrence. He underwent cryoablation for cT1N0M0 stage IA1 lung cancer at 52-year olds (Fig. 1a) and again because of local lung cancer recurrence at 56-year old (Fig. 1b). Chest computed tomography showed a progressively enlarging infiltration in segment 2 (Fig. 1c). A second local recurrence of lung cancer was diagnosed and robotic portal right upper lobectomy and mediastinal lymph node dissection were performed. Preoperative chest computed tomography with 3D image reconstruction also revealed a partial anomalous pulmonary venous return; V1–3 drained via the azygous vein into the superior vena cava, and the upper pulmonary vein did not drain into the left atrium.
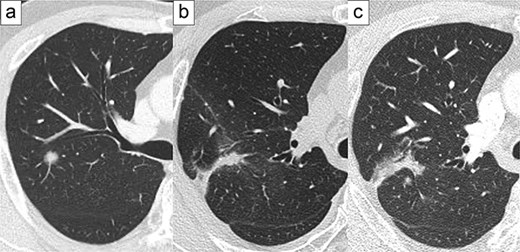
Representative images of preoperative computed tomography. Primary lung cancer at the age of 52 (a), first local recurrence at the age of 56 (b), and second local recurrence at the age of 58 (c).
Robotic portal surgery was performed under general and epidural anesthesia, with the patient placed in a decubitus position. Despite the presence of adhesions between the chest wall and upper lobe, an interlobar fissure between the upper and lower lobes resulting from cryoablation was observed. This fissure is divided using a stapler. Subsequently, the right upper bronchus and superior trunk of the pulmonary artery along with the interlobar fissure between the right upper and middle lobes were dissected using a surgical stapler. Finally, the aberrant pulmonary vein was dissected using a surgical stapler, and mediastinal lymph node dissection was performed at stations 2R and 4R. The postoperative course was uneventful, excluding the chylothorax, and the patient was discharged 13 days after surgical resection.
Microscopically, papillary adenocarcinoma, fibrosis, foreign body-type giant cells, and cholesterol clefts (Fig. 2) were observed. Therefore, the lesion was diagnosed as a local recurrence of adenocarcinoma post-cryoablation.
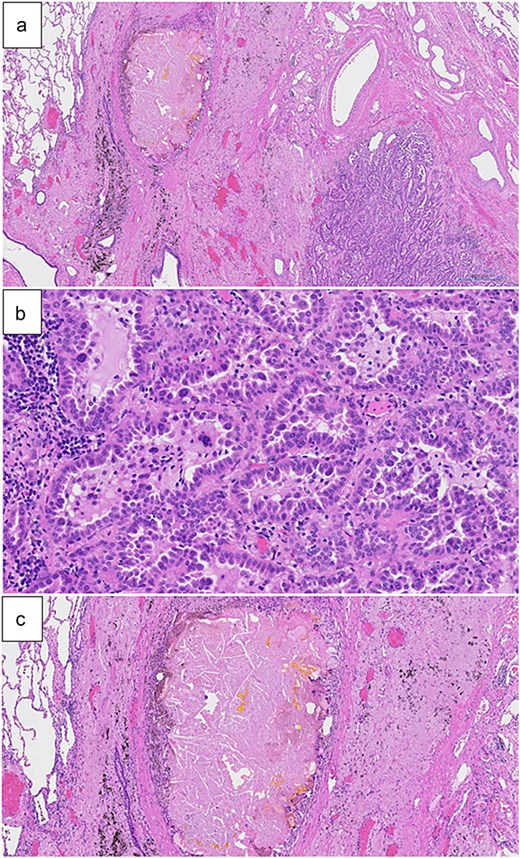
(a) Papillary adenocarcinoma, fibrosis, as well as foreign body-type giant cells and cholesterol clefts (hematoxylin and eosin staining, 2× magnification). (b) Papillary adenocarcinoma was dominantly observed (hematoxylin and eosin staining, 20× magnification). (c) Foreign body-type giant cells and cholesterol clefts were observed along with fibrosis (hematoxylin and eosin staining, 5× magnification).
Discussion
Surgical resection is the gold standard treatment for non-small cell lung cancer without distant metastasis [4]. In contrast, nonoperative therapies, including stereotactic body radiation therapy, radiofrequency, and cryoablation, have shown efficacy as local treatments for non-small cell lung cancer. In particular, the effectiveness and safety of cryoablation for lung cancers measuring <3 cm have been established. Nomori et al. reported that the recurrence rate post-cryoablation for T1N0M0 non-small cell lung cancer was 18%, with 8% of cases involving local recurrence and 10% involving metastasis [2]. In addition, local recurrence occurred in only 1 of 74 patients with lung cancers measuring <1.8 cm. The 3-year recurrence-free survival rates were 86% for tumors measuring <1.0 cm, 97% for tumors measuring 1.0 and 1.2 cm, and 92% for tumors measuring between 1.3 and 1.7 cm. These results are comparable with those of The JCOG0403 study, which focused on stereotactic body radiation therapy for operable T1N0M0 lung cancer [5]. The JCOG0403 study reported that the local control rate was 85% 3 years after treatment, and the recurrence-free survival rate was 55% with stereotactic body radiation therapy. In this case, although a good prognosis was expected with cryoablation due to the 12 mm size of the tumor, the patient experienced two instances of local recurrence. If cryoablation, a nonsurgical treatment option, is selected, the following points should be considered: First, it is difficult to evaluate lymph node metastasis pathologically without surgical resection. Second, local recurrence post-cryoablation is difficult to evaluate using follow-up computed tomography. Finally, the currently available evidence and observation period for previously reported cases were insufficient.
The pathological findings of the present case are valuable. As nonoperative treatment is selected for patients with early-stage lung cancer and low operative tolerance [3], it is difficult to perform surgical resection after recurrence. In the present case, a foreign body reaction was observed, characterized by the presence of foreign body-type giant cells and cholesterol clefts, which may have resulted from cryoablation. Thus, the observed adenocarcinoma was finally diagnosed as a local recurrence.
Conclusion
In conclusion, we report a case of robotic portal right upper lobectomy for a second recurrence post-cryoablation, with valuable pathological findings. Thus, cryoablation is a potential alternative to surgical resection in patients with low operative tolerance, however, further accumulation of clinical cases is warranted.
Conflict of interest statement
The authors have no conflicts of interest or financial ties to disclose.
Funding
None declared.

{kind=link}
{kind=link}