





Abstract
Penetrating cardiac trauma is one of the most critical emergency injuries, characterized by rapid progression and extremely high mortality. This article reports a case of a patient who sustained a gunshot wound that traversed the heart and lodged in the pericardial cavity, and was successfully rescued due to timely surgery.
Introduction
Penetrating cardiac trauma represents one of the most critical emergencies in trauma surgery, characterized by rapid progression and exceedingly high mortality. Although firearm-related penetrating cardiac injuries are relatively rare in countries and regions with strict gun control laws, they present a significant challenge to emergency care systems. The prognosis of such injuries highly depends on early, accurate diagnosis and timely surgical intervention. This article reports an exceptionally rare case of penetrating cardiac trauma caused by a projectile, in which the bullet perforated the heart and lodged within the pericardial sac. Through prompt diagnosis and emergent median sternotomy, the patient was successfully rescued and recovered favorably. This case report aims to discuss the clinical decision-making process involved in the management of such uncommon injuries and to provide valuable insights for handling similar rare emergencies.
Case report
A 61-year-old male was admitted to the emergency department after being struck by an unidentified object at home, followed by immediate onset of persistent and severe chest pain. There were no accompanying symptoms such as dizziness, headache, nausea, vomiting, or dyspnea. The patient was transferred via emergency medical services to a local hospital, where a chest computed tomography (CT) scan revealed pericardial effusion and an intracardiac foreign body. Due to limited treatment capabilities, the patient was subsequently referred to our emergency department.
Upon arrival, physical examination under norepinephrine infusion showed a blood pressure of 97/67 mmHg, a heart rate of 121 beats per minute, and a respiratory rate of 30 breaths per minute. A 0.5 × 1.0 cm spindle-shaped wound (Fig. 1A) was observed on the left anterior chest wall, with a small amount of bloody discharge. Breath sounds were diminished over the left lower lung, heart sounds were distant, and cardiac borders were enlarged. An urgent repeat chest CT demonstrated an irregular dense shadow with radial artifacts within the heart, suggestive of a cardiac foreign body, accompanied by moderate pericardial hemorrhage and moderate-to-large left hemothorax with associated atelectasis (Fig. 1B). Echocardiography confirmed a 12.5 × 11.8 mm hyperechoic mass in the pericardial cavity along with moderate pericardial effusion. Given the critical condition, an emergency thoracotomy was performed following evaluation by the cardiac surgery team (Video 1).
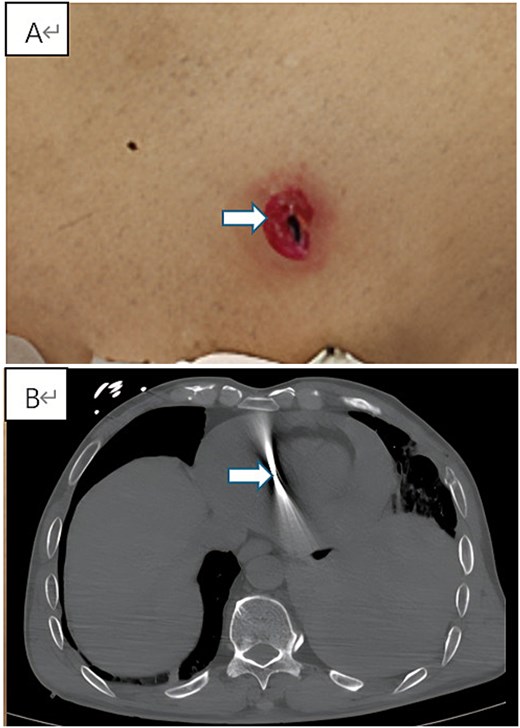
Preoperative clinical and imaging findings. (A) Photograph showing the spindle-shaped entry wound (0.5 × 1.0 cm) on the left anterior chest wall (indicated by arrow). (B) Axial view of contrast-enhanced chest CT revealing the metallic foreign body within the cardiac silhouette with radiopaque artifacts, accompanied by pericardial effusion and left hemothorax.
A median sternotomy was performed. Upon entering the mediastinum, active arterial bleeding was observed. The pericardium was subsequently incised, revealing ~300 ml of blood within the pericardial cavity. After evacuation of organized clots, a cylindrical metallic foreign body, ~1 cm in length, was identified and retrieved from within the clot (Fig. 2A). With continuous suction applied, two distinct cardiac lacerations with active oozing were identified on the lateral wall of the left ventricle (Fig. 2B). The heart was stabilized using a cardiac stabilizer, and the ruptures were primarily repaired without cardiopulmonary bypass. Subsequent exploration of the left lung revealed two lacerations on the lower lobe with ongoing bleeding. Approximately 1200 ml of blood was drained from the left pleural cavity, and the pulmonary lacerations were sutured. Meticulous exploration confirmed no additional injuries.
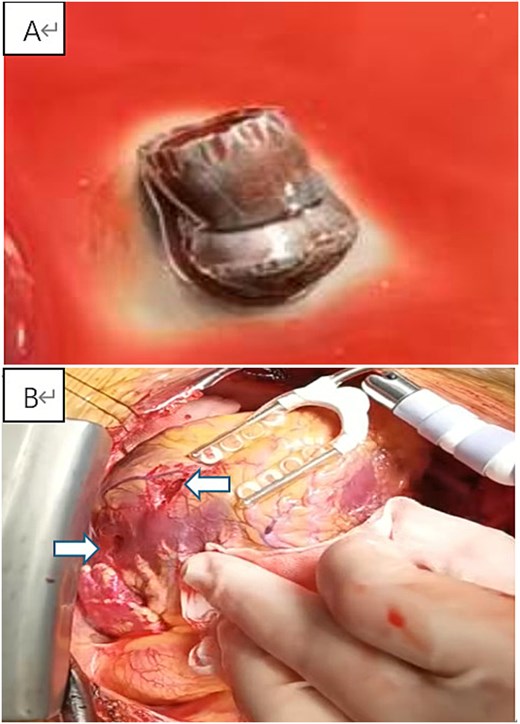
Intraoperative findings and retrieved foreign body. (A) The retrieved cylindrical metallic foreign body measuring ~1 cm in length. (B) Intraoperative view after median sternotomy, showing the cardiac laceration site on the left ventricular lateral wall.
The patient recovered well postoperatively, with stable vital signs and hemodynamics, and no significant arrhythmias or conduction disturbances were observed. He was discharged home 15 days after surgery and remained in stable condition at follow-up.
Discussion
In China, where firearm regulations are stringent, cardiac injuries caused by bullets are exceedingly rare. As a result, there is a lack of specific clinical guidelines for the management of gunshot-related thoracic injuries, and treatment principles are generally derived from those for general thoracic trauma, with the decision for emergency surgery based primarily on clinical presentation [1].
For hemodynamically stable patients, early imaging is essential to determine the bullet’s trajectory and position, which is critical for formulating a treatment plan. Although X-ray films can be used for bullet localization, CT imaging is preferred due to its ability to provide more detailed information regarding potential intrathoracic injuries [2]. Metallic foreign bodies such as bullets are contraindications for cardiac magnetic resonance imaging (MRI) because of their ferromagnetic properties [3]. Median sternotomy is generally the preferred approach in hemodynamically stable patients. While some studies advocate for subxiphoid pericardial window drainage as an initial step to relieve cardiac tamponade [4], this approach carries the risk of missing underlying myocardial or coronary injuries and may limit thorough exploration for associated injuries. In contrast, hemodynamically unstable or pulseless patients are typically managed via a left anterior lateral thoracotomy, which allows rapid access to the heart for internal cardiac massage, hemorrhage control, and decompression of cardiac tamponade [5].
In the present case, the patient remained relatively hemodynamically stable with fluid resuscitation and vasopressor support. Following prompt CT and echocardiographic evaluations, the patient underwent emergency thoracotomy and subsequently achieved a favorable recovery. Given the limited number of reported bullet-induced penetrating cardiac injuries in China and the consequent lack of established management experience, this case provides valuable insights into the management of such rare clinical entities.
Conclusion
Bullet-induced penetrating cardiac trauma is a devastating condition that poses a formidable challenge to clinicians. For hemodynamically stable patients, we advocate for early comprehensive imaging to minimize unforeseen complications. When surgery is indicated, a median sternotomy is the preferred initial approach, as it provides optimal exposure of the heart, thereby contributing to reduced mortality and postoperative complications.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}