





Abstract
We present a case in which the medial sectional bile duct (B4) drained the right hepatic duct. A 42-year-old man was referred to our hospital after an abdominal ultrasound during a medical check-up revealed a gallbladder polyp. Magnetic resonance cholangiopancreatography did not adequately depict the hepatic hilum bile ducts; therefore, drip infusion cholangiography with computed tomography was performed, which revealed that B4 drained the right hepatic duct. The patient subsequently underwent laparoscopic cholecystectomy. His post-operative course was uneventful, and he was discharged on post-operative Day 3. The confluence of B4 into the right hepatic duct is extremely rare. We report this case along with a brief review of the literature.
Introduction
Abnormalities in the course and confluence of the biliary tract are occasionally encountered. Thorough preoperative understanding of these anomalies is essential to determine the appropriate surgical procedure and prevent intraoperative biliary tract injury. Among intrahepatic bile ducts, the medial sectional bile duct (B4) is known to exhibit significant anatomical variability and various confluence patterns. We report a case of an extremely rare confluence pattern of B4, identified using drip infusion cholangiography with computed tomography (DIC-CT).
Case report
A 42-year-old man visited the surgical outpatient department for evaluation of a gallbladder polyp identified during a routine medical checkup. He had no notable medical history. Physical examination revealed no significant findings, and blood test results were unremarkable. Endoscopic ultrasonography demonstrated a round, elevated lesion measuring 9.5 mm in the gallbladder fundus. Computed tomography (CT) revealed a polypoid lesion with contrast enhancement measuring 10 mm in the same location. Magnetic resonance cholangiopancreatography was performed as part of the preoperative evaluation; however, visualization of the hilar bile ducts was insufficient. Therefore, DIC-CT was conducted to obtain a more detailed view of the biliary anatomy. It revealed that the left medial sectional bile duct (B4) drained the right hepatic duct (RHD) (Figs 1 and 2). A three-dimensional CT image, reconstructed using the Synapse Vincent volume analyzer (Fujifilm Holdings Corporation, Tokyo, Japan), revealed that the right posterior sectoral portal vein arose directly from the main portal vein (Fig. 3).
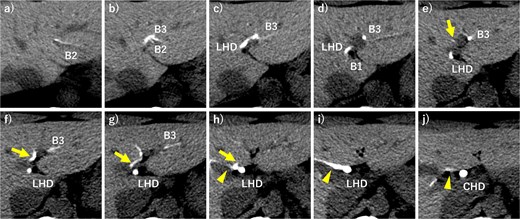
Axial view of drip infusion cholangiography with CT (DIC-CT). The left medial sectional bile duct (arrows) joined the right hepatic duct (arrowheads) (a–j) B1, bile duct of Segment 1; B2, bile duct of Segment 2; B3, bile duct of Segment 3; LHD, left hepatic duct; CHD, common hepatic duct.

Three-dimensional DIC-CT showing the left medial sectional bile duct (arrow) joined the right hepatic duct (arrowhead).
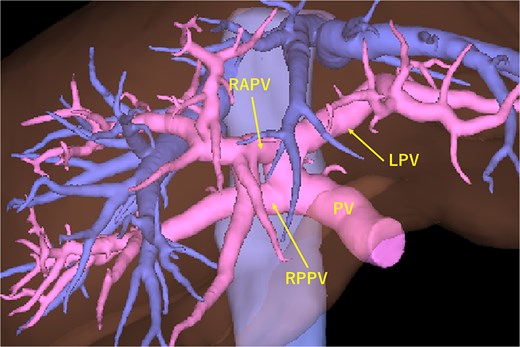
The portal vein diverges into the RPPV and the common trunk of the RAPV and LV. RAPV, right anterior sectoral portal vein; RPPV, right posterior sectoral portal vein; LPV, left portal vein; PV, portal vein.
The patient subsequently underwent laparoscopic cholecystectomy. His post-operative course was uneventful, and he was discharged 3 days after surgery. Histopathological diagnosis confirmed a cholesterol polyp.
Discussion
B4 is known to display a wide variety of confluence patterns [1–3], although it infrequently joins bile ducts other than the left intrahepatic ducts. Furusawa et al. [1] reviewed eight studies including 1973 patients and reported that B4 drained into the common hepatic duct, RHD, right anterior sectional duct, and right posterior sectional duct in 31 (1.6%), 153 (7.8%), 41 (2.1%), and 1 (0.05%) patients, respectively. Notably, only one study documented the 153 cases in which B4 drained into the RHD [3]. Furusawa et al. [1] speculated that this high incidence might be due to the use of direct cholangiography in that study, while other studies employed liver casts or resected specimens. To our knowledge, this is the first case report demonstrating B4 draining into the RHD on DIC-CT, a modality capable of visualizing both intrahepatic bile ducts and hepatic parenchyma.
Portal vein variations are often associated with biliary tract anomalies. In our case, a branching variation was observed in which the portal trunk divided into the right posterior sectoral portal vein and a common trunk comprising the right anterior sectoral portal vein and left portal veins. According to Kitami et al. [4], such variations occur in 6.0%–11.4% of cases. Furthermore, a RHD was observed in 79% of patients without portal vein variations but in only 45% of those with such variations, suggesting a significantly lower incidence in the latter group [4]. Furusawa et al. also reported that the incidence of B4 draining into the right-sided ducts or common hepatic duct was significantly higher in patients with portal vein variations [1]. When a portal vein anomaly is detected on CT, the possibility of a coexisting biliary tract anomaly should be carefully considered.
Although the variation in the present case did not affect the surgical procedure, caution is warranted to avoid B4 injury during procedures such as hemihepatectomy, anterior sectionectomy, medial sectionectomy, or Segment 5 resection in patients with B4 draining into ducts other than the left intrahepatic ones. Recognizing rare confluence patterns like this in advance is crucial for safe hepatobiliary surgery.
Conflict of interest statement
The authors declare no conflicts of interest for this article.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}