





Abstract
Gallbladder cancer is a rare and aggressive malignancy, representing 3%–4% of digestive cancers, and is often diagnosed at advanced stages, resulting in poor prognosis. This case report presents a 30-year-old woman with a 10-day history of right upper quadrant abdominal pain. Laboratory results revealed GB:12250, Hb:10.8 g/dL, Plt:538000, CRP:299 mg/L, with mild liver function disturbance (GGT:36, PAL:46, ASAT:13, ALAT:6, BT/BD:5/3). Imaging revealed a large mass at the gallbladder bed, suspected to be a tubulo-papillary intra-vesicular tumor, along with liver lesions and hydatid cysts. Exploratory laparotomy confirmed a ruptured gallbladder tumor, with histopathological findings indicating undifferentiated carcinoma. Cytology of the peritoneal fluid confirmed malignant cells. The tumor was staged as pT3NxMx, suggesting invasion of adjacent structures with uncertain lymph node and metastasis status. The patient received six cycles of adjuvant chemotherapy with gemcitabine and cisplatin. This report highlights the diagnostic challenges and aggressive nature of gallbladder cancer and presents a rare histological subtype with spontaneous rupture in a young patient, emphasizing the need for early detection and multidisciplinary management.
Introduction
Gallbladder cancer is an uncommon but highly lethal malignancy, accounting for approximately 3%–4% of all gastrointestinal cancers [1, 2]. It is characterized by aggressive biological behavior and is frequently diagnosed at advanced stages, contributing to the poor prognosis and limited treatment options. Due to its rarity, there is a lack of extensive clinical research compared to more common malignancies. Consequently, early detection remains difficult, and survival outcomes are often poor, particularly in patients with advanced disease at diagnosis [3].
Case presentation
A 30-year-old woman, gravida 2 para 2, presented with a 10-day history of right upper quadrant (RUQ) abdominal pain. She had no significant medical or surgical history and denied systemic symptoms such as fever, weight loss, or fatigue. On examination, she was afebrile and hemodynamically stable, with a WHO performance status of 1. Abdominal palpation revealed localized tenderness in the RUQ. Laboratory investigations revealed mild leukocytosis (12 250/μL), Hb:10.8 g/dL, Plt:538000, TP:64%, Na:132 mmol/L, K:4.1 mmol/L, CRP:299 mg/L. Liver function tests showed GGT:36 U/L, PAL:46 U/L, ASAT:13 U/L, ALAT:6 U/L, total bilirubin:5 mg/L, direct bilirubin:3 mg/L. Urea and creatinine were 0.2 and 3.6, respectively. Contrast-enhanced CT revealed a large mass in the gallbladder bed, suspected to be a tubulo-papillary intracholecystic neoplasm (ICPN) (Figs 1 and 2), with an associated angiomatous liver lesion in segment III, hydatid cysts, and mild ascites. Exploratory laparotomy was performed, revealing a ruptured gallbladder tumor with extension into adjacent liver tissue and abdominal wall, and free biliary stones within the peritoneal cavity (Fig. 3).
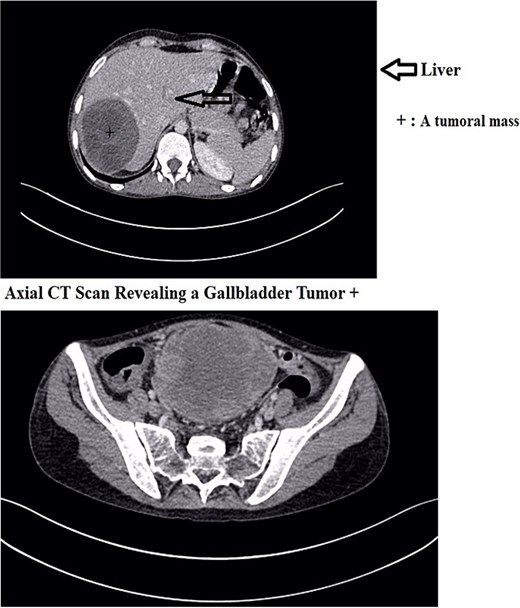
Axial CT scan revealing a gallbladder tumor with invasion of adjacent structures.
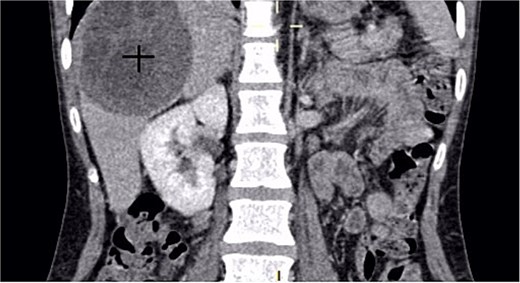
A coronal CT scan of the abdomen showing a large, well-defined hypodense mass in the right hepatic lobe.
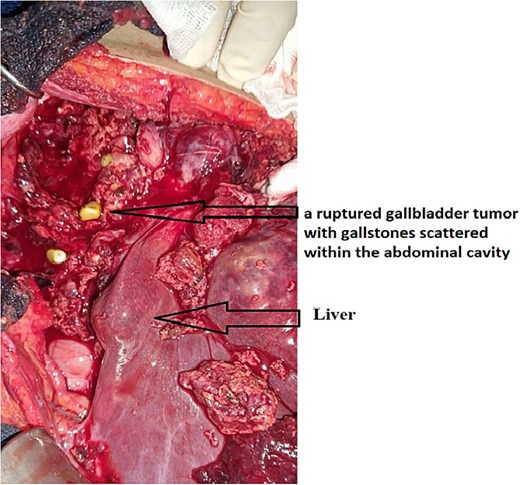
Intraoperative image showing a ruptured gallbladder tumor with gallstones scattered within the abdominal cavity. The tumor exhibits extensive invasion of adjacent tissues, emphasizing the aggressive nature of undifferentiated gallbladder carcinoma.
Operative intervention included:
Aspiration of ascitic fluid for cytological study (malignant cells detected).
Aspiration of ruptured tumor contents.
Section of the triangular ligament for mobilization of the right liver.
Peritoneal protection with hydrogen peroxide-soaked wicks.
Aspiration of hydatid cyst contents (rock water fluid and gelatinous membrane).
Resection of the protruding dome of the hydatid cyst.
Extensive lavage with hydrogen peroxide and saline.
Anterograde cholecystectomy with ligation and section of cystic duct and artery using 2/0 Vicryl (Fig. 4).
Hemostasis was achieved, and three drains were placed: two No. 28 subhepatic drains, one No. 26 drain in the Douglas pouch, and a Jackson-Pratt drain in the residual cyst cavity.
Closure with Vicryl 2 sutures and skin stapling. Textile count was correct.
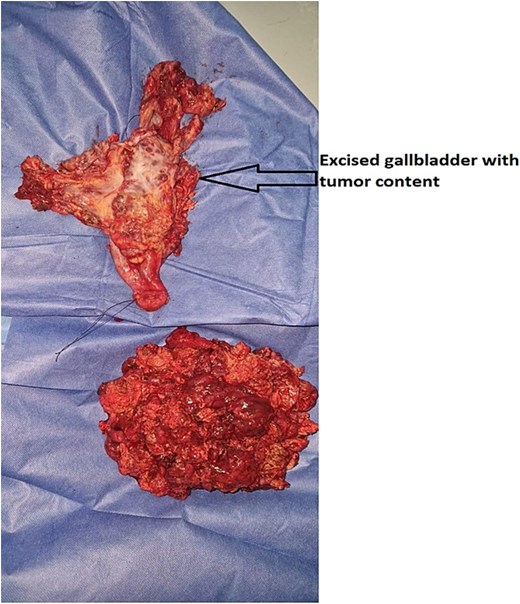
Surgical specimen following cholecystectomy, showing the excised gallbladder with undifferentiated carcinoma and tumor content. The specimen exhibits extensive tumor invasion with irregular, friable, and hemorrhagic tissue, consistent with an aggressive malignancy.
Histopathological findings
Microscopic evaluation revealed a poorly differentiated neoplasm composed of pleomorphic cells arranged in solid sheets and nests, with high nuclear-cytoplasmic ratio, prominent nucleoli, and brisk mitotic activity. Extensive necrosis was present. Immunohistochemical staining was positive for cytokeratin AE1/AE3 and vimentin, while negative for CK7, CK20, HepPar-1, and chromogranin, supporting the diagnosis of undifferentiated carcinoma. Vascular emboli were identified, and residual tumor cells were present at the resection margin, consistent with an R1 resection. The tumor was staged as pT3NxMx (Figs 5–8).
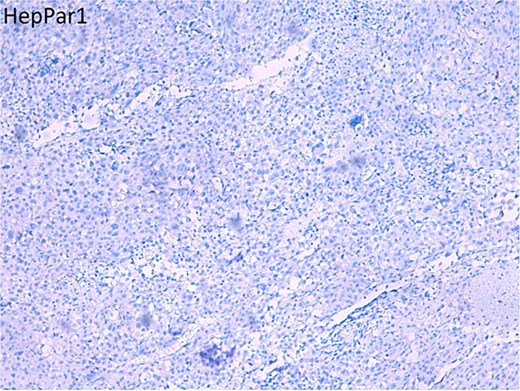
Histopathological section stained for HepPar-1, showing negative immunoreactivity in tumor cells.
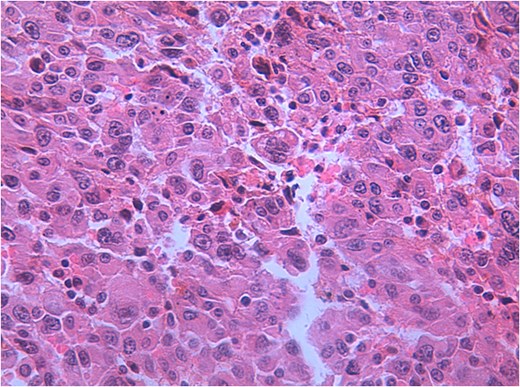
Hematoxylin and eosin (H&E) staining of the gallbladder tumor showing highly pleomorphic tumor cells with abundant eosinophilic cytoplasm, prominent nucleoli, and frequent mitotic figures, consistent with undifferentiated carcinoma.
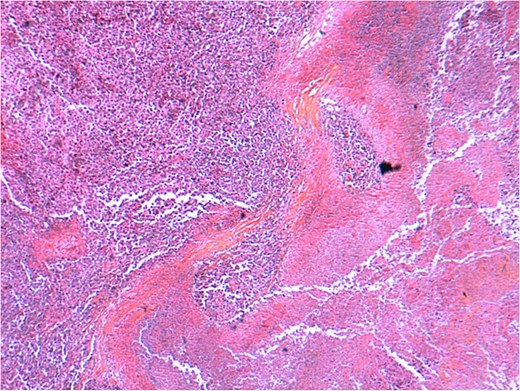
Histopathological examination of the gallbladder tumor (H&E stain) showing a highly undifferentiated carcinoma with extensive necrosis and inflammatory infiltrates. The tumor exhibits irregular architecture with areas of stromal reaction and vascular invasion.
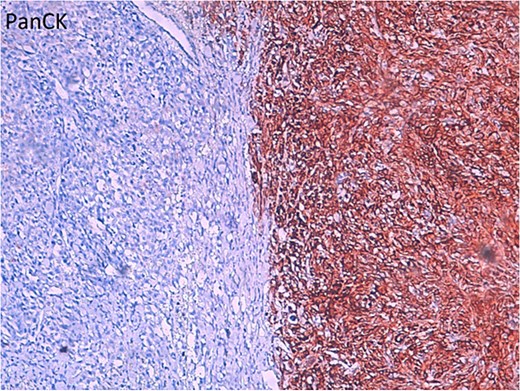
Immunohistochemical staining for Pan-Cytokeratin (PanCK) demonstrating strong positivity in the carcinoma cells (brown staining), highlighting their epithelial origin. The left side of the image shows a negative-staining area, possibly representing tumor necrosis or nonepithelial components.
Follow-up
Postoperatively, the patient recovered without immediate complications. Peritoneal fluid cytology confirmed malignant cells. The patient underwent six cycles of adjuvant chemotherapy with gemcitabine and cisplatin. Surveillance included regular clinical examinations, liver function tests, tumor markers (CEA, CA19-9), and thoracoabdominal-pelvic CT scans every three to 6 months. Follow-up imaging revealed stable disease after 2 years. At the latest evaluation, the patient remained clinically stable with no radiologic evidence of new metastasis.
Discussion
Gallbladder cancer is a rare entity that presents significant diagnostic and therapeutic challenges due to its nonspecific symptoms and typically late-stage diagnosis [1, 3]. Despite accounting for only a small proportion of digestive tract malignancies, it has a disproportionately poor prognosis. Adenocarcinoma is the predominant histological type (accounting for ~90%) and can present in several morphological variants, including infiltrative, papillary, and mucinous forms [4]. Papillary adenocarcinomas tend to have better outcomes when polypoid and noninvasive. However, undifferentiated carcinoma of the gallbladder, as seen in our case, is exceedingly rare. Risk factors include gallstones, chronic inflammation, infections, hormonal factors, and congenital biliary anomalies [5–7]. Imaging modalities such as CT, MRI, and PET/CT are critical for staging, but definitive diagnosis often requires histology [8]. Tumor markers are useful for monitoring but lack specificity.
Clinical significance
This case is noteworthy due to the rare occurrence of undifferentiated gallbladder carcinoma in a young female without conventional risk factors, accompanied by spontaneous rupture, biliary peritoneal seeding, and concurrent hydatid disease. To our knowledge, very few cases in the literature describe this unique constellation of findings. It highlights the necessity for high clinical suspicion even in young patients with atypical biliary presentations and reinforces the aggressive behavior of undifferentiated gallbladder tumors.
Conclusion
Gallbladder cancer remains a rare and often fatal malignancy, particularly in its undifferentiated form. This case underscores an unusual presentation in a young adult with spontaneous tumor rupture and vascular invasion. Multidisciplinary collaboration, careful operative planning, and long-term surveillance are vital. Further studies focusing on early diagnostic markers and targeted therapies are urgently needed to improve outcomes in such aggressive variants.
Author contributions
Slimi Youness (have written the article, have consulted the patient, and prepared the patient for surgery and participated in the surgery), Mahmoudi Mohammed (have helped writing the article, data collection), Meziane Mohammed (have helped collecting data), Akouh Nada (have helped collecting data), Guellil Abdelali (supervised the writing of manuscript), Jabi Rachid (supervised the writing of manuscript), Bennani Amal (have posed the radiological diagnosis), Bouziane Mohamed (have supervised the writing of the paper, and has been the leader surgeon of the case).
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}